
Value of Ki-67 index in evaluating the prognosis of adrenocortical carcinoma after surgery
-
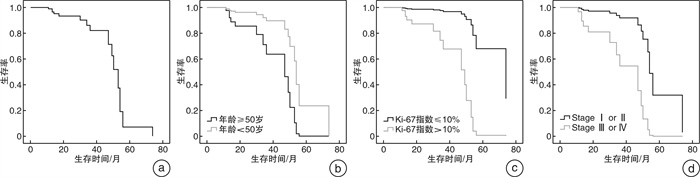
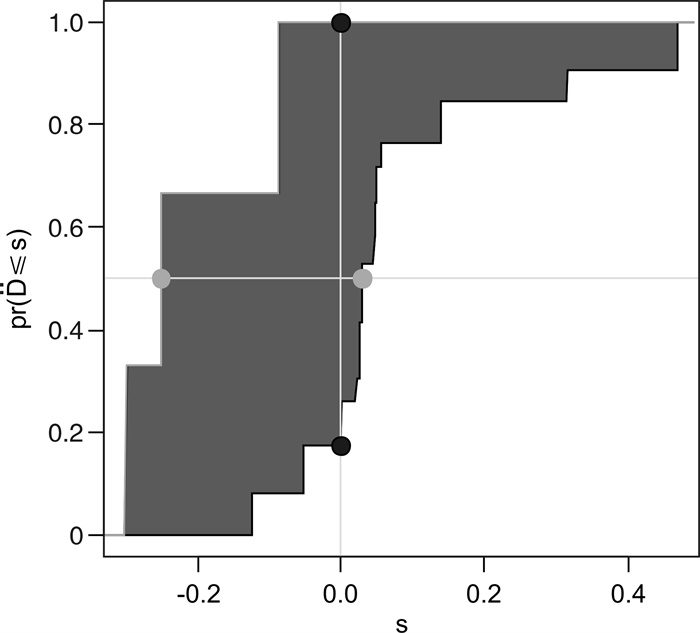
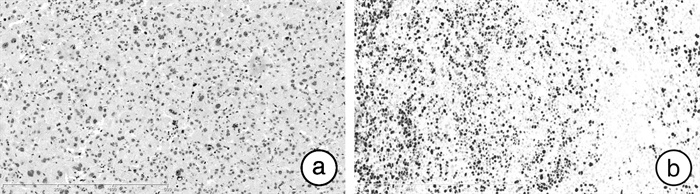
摘要: 目的 探索Ki-67指数对肾上腺皮质癌(ACC)术后预后的预测价值。方法 分析2010年1月—2018年1月经术后病理证实的40例ACC患者临床及病理数据。将其分为存活组和死亡组,根据疾病分期、Ki-67免疫组织化学染色和随访结果,利用Cox比例风险回归模型分析Ki-67指数及其联合肿瘤分期对ACC术后的预后影响。结果 共有40例患者纳入研究,存活组患者24例,Ⅲ~Ⅳ期肿瘤分期为33.3%,Ki-67平均指数为17.2%,Ki-67指数>10%者占54.2%。死亡组患者16例,Ⅲ~Ⅳ期肿瘤分期为56.3%,Ki-67平均指数为34.2%,>10%者占93.8%。单因素分析发现,性别、肿瘤直径、分期、Ki-67指数均是影响患者预后的危险因素。当Ki-67指数>10%与≤10%对比HR=10.30(P=0.026)。经多因素分析,Ki-67指数是影响患者预后的独立危险因素,Ki-67指数>10%与≤10%对比HR=13.33(P=0.02)。通过将Ki-67指数与分期联合评估预后价值,C-index显著提高为0.84(95%CI:0.67~1.02),综合判别改善指数(IDI)为0.291(P=0.013)。结论 Ki-67指数是ACC术后患者预后的独立影响因素,其与肿瘤分期联合可以显著提高ACC患者术后预后情况预测能力的评估。Abstract: Objective To explore the predictive value of Ki-67 index for the prognosis of adrenocortical carcinoma (ACC) after surgery.Methods The clinical and pathological data of 40 ACC patients confirmed by postoperative pathology from January 2010 to January 2018 were retrospectively analyzed. They were divided into survival group and death group. Based on the disease stage, Ki-67 immunohistochemical staining and follow-up results, the Cox proportional hazard regression model was used to analyze the influence of Ki-67 index and tumor stage on the prognosis of ACC.Results A total of 40 patients were included in the study; 24 were survival patients; tumor stage Ⅲ-Ⅳ accounted for 33.3%;the average Ki-67 index was 17.2%, and those with a Ki-67 index > 10% accounted for 54.2%. There were 16 patients who died. The proportion of stage Ⅲ-Ⅳ tumors was 56.3%, the average Ki-67 index was 34.2%, and those with > 10% accounted for 93.8%. Univariate analysis found that gender, tumor diameter, stage, and Ki-67 index are risk factors that affect the prognosis of patients. When Ki-67 index > 10%, HR of ≤10% is 10.30 (P=0.026). For multivariate analysis, Ki-67 index is an independent risk factor for the prognosis of patients. Compared to Ki-67 index≤10%, HR of Ki-67 index > 10% is 13.33 (P=0.02). When the prognostic value was evaluated by combining the Ki-67 index and stage, the C-index was significantly improved to 0.84 (95%CI: 0.67- 1.02), and the IDI was 0.291 (P=0.013).Conclusion Ki-67 index is an independent factor influencing the prognosis of patients with ACC after surgery. The combination of Ki-67 index and tumor stage can significantly improve the evaluation of the prognostic ability of ACC patients after surgery.
-
Key words:
- adrenocortical carcinoma /
- Ki-67 index /
- prognostic factors
-

-
表 1 40例ACC患者一般资料
例(%) 分组 存活组(n=24) 死亡组(n=16) 平均肿瘤直径/cm 8.20 10.91 平均随访时间/月 32.3(5~101) 37.4(11~74) 性别 男 8(33.33) 13(81.25) 女 16(66.67) 3(18.75) 年龄 < 50岁 12(50.00) 11(68.75) ≥50岁 12(50.00) 5(31.25) 直径/cm ≤10 20 6 >10 4 10 分期 Ⅰ~Ⅱ 16(66.67) 7(43.75) Ⅲ~Ⅳ 8(33.33) 9(56.25) Ki-67指数 ≤10% 11(45.83) 1(6.25) >10% 13(54.17) 15(93.75)  下载: 导出CSV
下载: 导出CSV
表 2 ACC患者总生存的单因素和多因素 Cox 比例风险回归分析
单因素分析 多因素分析 HR P HR P 性别 2.38 0.009 / 0.342 年龄 / 0.976 / / 直径 5.01 0.004 / 0.359 分期 7.22 0.002 7.11 0.004 Ki-67指数 10.30 0.026 13.33 0.020
下载: 导出CSV
-
[1] Fassnacht M, Dekkers OM, Else T, et al. European Society of Endocrinology Clinical Practice Guidelines on the management of adrenocortical carcinoma in adults, in collaboration with the European Network for the Study of Adrenal Tumors[J]. Eur J Endocrinol, 2018, 179(4): G1-G46. doi: 10.1530/EJE-18-0608
[2] Kiesewetter B, Riss P, Scheuba C, et al. Management of adrenocortical carcinoma: are we maKing progress?[J]. Ther Adv Med Oncol, 2021, 13: 17588359211038409.
[3] Cantini G, Fei L, Canu L, et al. Circulating Fascin 1 as a Promising Prognostic Marker in Adrenocortical Cancer[J]. Front Endocrinol(Lausanne), 2021, 12: 698862. doi: 10.3389/fendo.2021.698862
[4] Mete O, Gucer H, Kefeli M, et al. Diagnostic and Prognostic Biomarkers of Adrenal Cortical Carcinoma[J]. Am J Surg Pathol, 2018, 42(2): 201-213. doi: 10.1097/PAS.0000000000000943
[5] Parianos C, Kyriakopoulos G, KostaKis ID, et al. Adrenocortical Cancer: A 20-Year Experience of a Single Referral Center in Prognosis and Outcomes[J]. Horm Metab Res, 2021, 53(11): 709-716. doi: 10.1055/a-1666-9026
[6] Martins-Filho SN, Almeida MQ, Soares I, et al. Clinical Impact of Pathological Features Including the Ki-67 Labeling Index on Diagnosis and Prognosis of Adult and Pediatric Adrenocortical Tumors[J]. Endocr Pathol, 2021, 32(2): 288-300. doi: 10.1007/s12022-020-09654-x
[7] Puglisi S, Perotti P, Cosentini D, et al. Decision-maKing for adrenocortical carcinoma: surgical, systemic, and endocrine management options[J]. Expert Rev Anticancer Ther, 2018, 18(11): 1125-1133. doi: 10.1080/14737140.2018.1510325
[8] Babinska A, Peksa R, Wisniewski P, et al. Diagnostic and prognostic role of SF1, IGF2, Ki67, p53, adiponectin, and leptin receptors in human adrenal cortical tumors[J]. J Surg Oncol, 2017, 116(3): 427-433. doi: 10.1002/jso.24665
[9] Kieler M, Mullauer L, Koperek O, et al. Analysis of 10 Adrenocortical Carcinoma Patients in the Cohort of the Precision Medicine Platform MONDTI[J]. Oncology, 2018, 94(5): 306-310. doi: 10.1159/000486678
[10] Jouinot A, Bertherat J. MANAGEMENT OF ENDOCRINE DISEASE: Adrenocortical carcinoma: differentiating the good from the poor prognosis tumors[J]. Eur J Endocrinol, 2018, 178(5): R215-R230. doi: 10.1530/EJE-18-0027
[11] Dinnes J, Bancos I, Ferrante di Ruffano L, et al. MANAGEMENT OF ENDOCRINE DISEASE: Imaging for the diagnosis of malignancy in incidentally discovered adrenal masses: a systematic review and meta-analysis[J]. Eur J Endocrinol, 2016, 175(2): R51-R64. doi: 10.1530/EJE-16-0461
[12] Else T, Kim AC, Sabolch A, et al. Adrenocortical carcinoma[J]. Endocr Rev, 2014, 35(2): 282-326. doi: 10.1210/er.2013-1029
[13] Leong D, Nyantoro M, Shedzad H, et al. Management of adrenocortical carcinoma in Western Australia: a perspective over 14 years[J]. ANZ J Surg, 2021, 91(1-2): 62-67. doi: 10.1111/ans.16111
[14] Ball MW, Hemal AK, Allaf ME. International Consultation on Urological Diseases and European Association of Urology International Consultation on Minimally Invasive Surgery in Urology: laparoscopic and robotic adrenalectomy[J]. BJU Int, 2017, 119(1): 13-21. doi: 10.1111/bju.13592
[15] Kroiss M, Deutschbein T, Schlotelburg W, et al. Treatment of Refractory Adrenocortical Carcinoma with Thalidomide: Analysis of 27 Patients from the European Network for the Study of Adrenal Tumours Registry[J]. Exp Clin Endocrinol Diabetes, 2019, 127(9): 578-584. doi: 10.1055/a-0747-5571
[16] Terzolo M, Angeli A, Fassnacht M, et al. Adjuvant mitotane treatment for adrenocortical carcinoma[J]. N Engl J Med, 2007, 356(23): 2372-2380. doi: 10.1056/NEJMoa063360
[17] Paragliola RM, Torino F, Papi G, et al. Role of Mitotane in Adrenocortical Carcinoma-Review and State of the art[J]. Eur Endocrinol, 2018, 14(2): 62-66. doi: 10.17925/EE.2018.14.2.62
[18] Feliu C, Cazaubon Y, Guillemin H, et al. Therapeutic drug monitoring of mitotane: Analytical assay and patient follow-up[J]. Biomed Chromatogr, 2017, 31(11).
-
图(3)
表(2)
计量
- 文章访问数: 926
- PDF下载数: 547
- 施引文献: 0