
Evaluation of the clinical value of pelvic floor MRI in female stress urinary incontinence
-
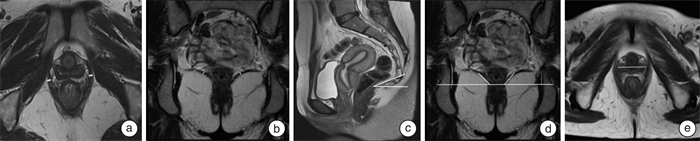
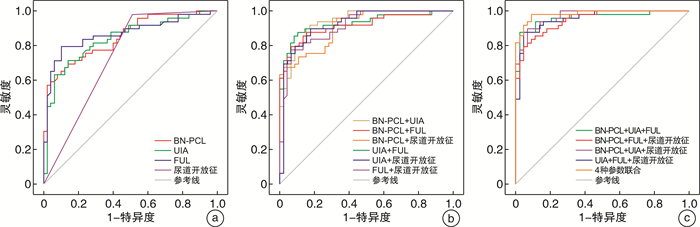
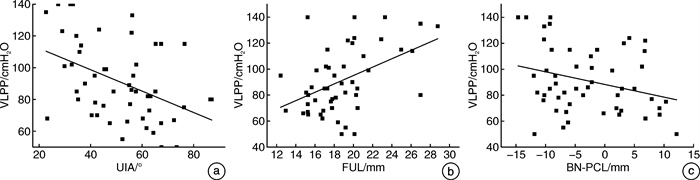
摘要: 目的 基于动静态盆底MRI评估女性压力性尿失禁(stress urinary incontinence,SUI)盆底结构的变化,并探讨盆底MRI相关参数对女性SUI的预测价值。方法 前瞻性收集2020年7月—2022年3月于郑州大学第一附属医院经尿动力学检查诊断为SUI患者51例作为SUI组,选取同期年龄与之相匹配的健康志愿者49例作为对照组。所有患者及健康志愿者均行动静态盆底MRI扫描,在静态和动态最大力排相上观察有无膀胱颈漏斗及尿道开放征,并测量尿道倾斜角(UIA)、膀胱颈(BN)到耻骨尾骨线(PCL)的距离(BN-PCL)、尿道中段括约肌(横纹肌和平滑肌)厚度以及功能尿道长度(FUL)、双侧耻骨直肠肌(PRM)厚度、髂尾肌(ICM)厚度、肛提肌裂孔最大横径(LHW)、提肛板角(LPA)、髂尾角(ICA)等。分析2组动静态MRI测量值的差异,筛选影响SUI发生的参数,建立ROC曲线并计算相关参数的AUC值、灵敏度、特异度、最佳阈值,并分析相关参数与尿动力学检查漏尿点压力(VLPP)的相关性。结果 膀胱尿道相关参数中,SUI组的尿道中段横纹肌厚度、静态及动态最大力排相FUL值、静态及动态最大力排相BN-PCL值均较对照组小(P< 0.05);SUI组静态及动态最大力排相UIA值、UIA差值、FUL差值及BN-PCL差值均较对照组大(P< 0.05);SUI组静态及动态最大力排相膀胱颈漏斗征阳性率、动态最大力排相尿道开放征阳性率均大于对照组。肛提肌相关参数中,SUI组双侧PRM厚度均较对照组小(P< 0.05);SUI组LHW、静态及动态最大力排相LPA值、LPA差值均较对照组增大(P< 0.05)。动态最大力排相BN-PCL、UIA、FUL和尿道开放征的AUC值分别为0.849、0.838、0.857及0.735;灵敏度分别为81.6%、78.4%、80.2%、49.0%;特异度分别为71.4%、75.5%、77.6%、98.0%。以上4个盆底参数分别进行2个、3个和4个参数组合进行ROC曲线分析时,任意参数联合诊断效能均大于单项参数,其中BN-PCL+UIA+FUL参数联合评估是预测SUI的最佳指标。动态最大力排相UIA与VLPP呈负相关(rs=-0.431,P< 0.05);动态最大力排相FUL与VLPP呈正相关(rs=0.395,P< 0.05)。结论 MRI检查可以清楚显示盆底结构变化,利用盆底多种参数联合应用分析,能够明显提高对SUI的预测效能,并为进一步探讨女性SUI发病机制提供依据。Abstract: Objective To evaluate the changes of pelvic floor structure of female stress urinary incontinence (SUI) based on dynamic and static pelvic floor MRI, and to explore the predictive value of pelvic floor MRI-related parameters for SUI.Methods From July 2020 to March 2022, 51 patients with SUI diagnosed by urodynamic examination in First Affiliated Hospital of Zhengzhou University were prospectively collected as the SUI group, and 49 age-matched healthy volunteers were selected as the control group during the same period. All patients and healthy volunteers were scanned by static and dynamic pelvic floor MRI. The presence of bladder neck funneling and urethral opening sign were observed on static and maximal strain phase of dynamic MRI, and the urethral inclination angle (UIA), bladder neck (BN) to pubococcygeal line (PCL) distance (BN-PCL), midurethral sphincter (striated muscle and smooth muscle) thickness and functional urethral length (FUL), bilateral puborectalis muscle (PRM) thickness, iliococcygeus muscle (ICM) thickness, levator hiatus width (LHW), levator plate angle (LPA), iliococcygeal angle (ICA), etc. The differences between the two groups of dynamic and static MRI measurements were analyzed, then parameters affecting the occurrence of SUI were selected. The ROC curve was established and the AUC value, sensitivity, specificity and optimal threshold of relevant parameters were calculated. The correlation between relevant parameters and Valsalva leak point pressure (VLPP) was analyzed.Results Among the parameters related to the bladder and urethra: the thickness of the striated muscle in the middle urethra, the FUL value of the static and maximal strain phase of dynamic MRI, and the BN-PCL value of the static and maximal strain phase of dynamic MRI of the SUI group were significantly decreased (P< 0.05). The UIA and the difference of UIA, FUL and BN-PCL values between static status and maximal strain phase were significantly increased (P< 0.05). The positive rate of bladder neck funnel in static status and maximal strain phase, urethral opening in maximal strain phase of SUI group increased significantly. Among the parameters related to the levator ani muscle: the bilateral PRM thickness in the SUI group were smaller than that in the control group (P< 0.05). The LHW, the static and maximal strain phase LPA value and LPA difference in the SUI group were larger than those in the control group (P< 0.05). The AUC values of BN-PCL, UIA, FUL and urethral opening sign on maximal strain phase of dynamic MRI were 0.849, 0.838, 0.857 and 0.735, respectively; the sensitivity were 81.6%, 78.4%, 80.2%, 49.0%; the specificity were 71.4%, 75.5%, 77.6%, and 98.0%, respectively. When the above four pelvic floor parameters were analyzed with two, three and four parameters, the combined diagnostic efficiency of any parameter was greater than a single parameter, among which the combined evaluation of BN-PCL+UIA+FUL parameters was the best index to predict SUI. The UIA on maximal strain phase of dynamic MRI was negatively correlated with VLPP (rs=-0.431,P< 0.05), while the FUL on maximal strain phase was positively correlated with VLPP (rs=0.395,P< 0.05).Conclusion MRI examination can clearly show the structural changes of the pelvic floor. The combined application and analysis of multiple parameters of the pelvic floor can significantly improve the prediction efficiency of SUI, and provide a basis for further exploring the pathogenesis of female SUI.
-
Key words:
- magnetic resonance imaging /
- stress urinary incontinence /
- levator ani muscle /
- urethra /
- diagnosis
-

-
表 1 SUI组与对照组临床资料比较
例(%),X±S,M(P25,P75) 项目 SUI组(51例) 对照组(49例) t/Z/χ2 P值 年龄/岁 52.88±10.84 51.22±6.44 0.934 0.353 BMI/(kg/m2) 25.03±3.35 22.71±2.51 4.384 < 0.001 绝经情况 0.918 0.632 未绝经 12(23.53) 12(24.49) 围绝经 11(21.57) 7(14.29) 绝经 28(54.90) 30(61.22) 产次 2(2,3) 2(2,2) -1.120 0.263 分娩方式 阴道次数 2(1,2) 2(1,2) -0.098 0.922 剖宫产次数 0(0,1) 0(0,1) -9.140 0.361  下载: 导出CSV
下载: 导出CSV
表 2 SUI组与对照组动静态MRI膀胱尿道相关参数比较
X±S,M(P25,P75) 参数 SUI组(51例) 对照组(49例) t/Z值 P值 尿道中段横纹肌厚度(静态) 2.05±0.37 2.46±0.36 -5.640 < 0.001 尿道中段平滑肌肌厚度(静态) 4.19±0.61 4.30±0.78 -0.816 0.417 FUL(静态) 26.32±2.69 29.65±2.42 -6.478 < 0.001 FUL(动态最大力排相) 18.04±3.48 23.97±4.09 -7.809 < 0.001 FUL(差值) 8.27±3.81 5.67±3.47 -3.558 0.001 UIA(静态) 6.21(-6.12,9.95) -5.37(-10.26,4.54) -3.075 0.002 UIA(动态最大力排相) 51.07±19.15 28.13±15.76 6.522 < 0.001 UIA(差值) 50.96(41.60,69.19) 30.11(22.99,35.35) -5.220 < 0.001 BN-PCL(静态) 16.01±6.13 20.31±4.23 -4.061 < 0.001 BN-PCL(动态最大力排相) -3.65(-9.27,5.01) 13.21(4.78,15.55) -6.127 < 0.001 BN-PCL(差值) 17.49(13.97,23.12) 7.87(6.26,13.31) -5.130 < 0.001
下载: 导出CSV
表 3 SUI组与对照组膀胱漏斗及尿道开放征阳性率比较
例(%) 组别 例数 静态膀胱颈漏斗征 动态最大力排相膀胱颈漏斗征 静态尿道开放征 动态最大力排相尿道开放征 + - + - + - + - SUI组 51 41(80.39) 10(19.61) 51(100.00) 0 0 51(100.00) 25(49.02) 26(50.98) 对照组 49 21(42.86) 28(57.14) 25(51.02) 24(48.98) 0 49(100.00) 1(2.04) 48(97.96) χ2值 14.944 32.868 - 28.666 P值 < 0.001 < 0.001 - < 0.001
下载: 导出CSV
表 4 SUI组与对照组动静态MRI肛提肌相关参数比较
X±S,M(P25,P75) 参数 SUI组(51例) 对照组(49例) t/Z值 P值 PRM-L(静态) 6.24±1.91 7.21±2.18 -2.358 0.020 PRM-R(静态) 5.56±1.70 6.67±1.88 -3.095 0.003 ICM-L(静态) 3.37±1.13 3.62±1.02 -1.135 0.259 ICM-R(静态) 3.33±1.06 3.61±1.01 -1.397 0.166 LHW(静态) 35.97±4.60 32.20±3.39 4.645 < 0.001 ICA-L(静态) 38.01±7.15 37.26±8.50 0.474 0.637 ICA-R(静态) 37.87±8.03 36.41±7.99 0.914 0.363 LPA(静态) 35.86±6.75 31.16±4.19 4.198 < 0.001 LPA(动态最大力排相) 50.87±9.51 41.58±5.37 6.037 < 0.001 LPA(差值) 13.27(8.96,22.11) 10.01(7.99,12.09) -2.786 0.005
下载: 导出CSV
表 5 影响SUI发生的盆底参数logistic回归分析结果
参素 B SE P值 OR OR(95%CI) 下限 上限 BN-PCL(动态最大力排相) -0.427 0.167 0.011 1.532 1.104 2.128 UIA(动态最大力排相) 0.188 0.074 0.017 0.837 0.724 0.968 FUL(动态最大力排相) -0.393 0.173 0.020 1.409 1.179 1.685 尿道开放征(动态最大力排相) 2.914 1.179 0.016 11.889 1.470 150.821
下载: 导出CSV
表 6 盆底MRI参数诊断SUI的ROC曲线分析结果
参素 AUC值 最佳阈值 灵敏度 特异度 约登指数 BN-PCL(动态最大力排相) 0.849 -6.85 81.6% 71.4% 0.553 UIA(动态最大力排相) 0.838 35.58 78.4% 75.5% 0.539 FUL(动态最大力排相) 0.857 22.51 80.2% 77.6% 0.637 尿道开放征(动态最大力排相) 0.735 - 49.0% 98.0% 0.470 BN-PCL+UIA 0.936 0.476 84.4% 86.0% 0.675 BN-PCL+FUL 0.918 0.463 84.7% 85.2% 0.702 BN-PCL+尿道开放征 0.910 0.356 75.1% 92.1% 0.641 UIA+FUL 0.929 0.571 90.9% 84.5% 0.754 UIA+尿道开放征 0.923 0.464 82.0% 88.1% 0.729 FUL+尿道开放征 0.911 0.585 85.9% 79.8% 0.678 BN-PCL+UIA+FUL 0.962 0.786 97.9% 84.7% 0.781 BN-PCL+UIA+尿道开放征 0.966 0.649 93.6% 87.2% 0.765 UIA+FUL+尿道开放征 0.955 0.752 94.2% 82.5% 0.781 BN-PCL+FUL+尿道开放征 0.951 0.642 92.6% 83.7% 0.689 4种参数联合 0.982 0.469 90.4% 89.3% 0.831
下载: 导出CSV
-
[1] Liu XH, Hu H, Zhang WY, et al. Repeat mid-urethral sling in management of recurrent or persistent stress urinary incontinence[J]. Chin Med J(Engl), 2020, 133(3): 367-368. http://d.wanfangdata.com.cn/periodical/zhcmj202003015
[2] Legendre G, Fritel X, Panjo H, et al. Incidence and remission of stress, urge, and mixed urinary incontinence in midlife and older women: A longitudinal cohort study[J]. Neurourol Urodyn, 2020, 39(2): 650-657. doi: 10.1002/nau.24237
[3] 崔伟, 王策正, 车梓, 等. 经阴手术治疗女性盆腔器官脱垂合并隐匿性压力性尿失禁临床分析[J]. 临床泌尿外科杂志, 2021, 36(10): 820-822, 826. doi: 10.13201/j.issn.1001-1420.2021.10.013
[4] 中华医学会放射学分会MR学组. 女性盆底功能障碍性疾病的MRI技术与报告规范[J]. 中华放射学杂志, 2022, 56(1): 16-24.
[5] Falah-Hassani K, Reeves J, Shiri R, et al. The pathophysiology of stress urinary incontinence: a systematic review and meta-analysis[J]. Int Urogynecol J, 2021, 32(3): 501-552. doi: 10.1007/s00192-020-04622-9
[6] 李晓伟, 王建六. 尿失禁的病因和发病机制[J]. 实用妇产科杂志, 2018, 34(3): 162-164. https://www.cnki.com.cn/Article/CJFDTOTAL-SFCZ201803003.htm
[7] Pereira TA, D'ancona C, Cândido EC, et al. Prevalence of LUTS and urodynamics results in obese women[J]. Neurourol Urodyn, 2022, 41(1): 468-474. doi: 10.1002/nau.24852
[8] Qi X, Shan J, Peng L, et al. The effect of a comprehensive care and rehabilitation program on enhancing pelvic floor muscle functions and preventing postpartum stress urinary incontinence[J]. Medicine(Baltimore), 2019, 98(35): e16907. http://pubmed.ncbi.nlm.nih.gov/31464923/
[9] 张静, 杨子涛, 张艳, 等. 静态和动态盆底MRI及扩散张量成像评估女性压力性尿失禁患者尿道形态及功能的应用研究[J]. 中华放射学杂志, 2022, 56(4): 411-417.
[10] Li M, Wang B, Liu X, et al. MR defecography in the assessment of anatomic and functional abnormalities in stress urinary incontinence before and after pelvic reconstruction[J]. Eur J Radiol, 2020, 126: 108935. doi: 10.1016/j.ejrad.2020.108935
[11] Ansquer Y, Fernander P, Aimot S, et al. MRI urethrovesical junction mobility is associated with global pelvic floor laxity in female stress incontinence[J]. Acta Obstet Gynecol Scand, 2007, 86(10): 1243-1250. http://onlinelibrary.wiley.com/doi/10.1080/00016340701550990/abstract
[12] 李敏, 王飚, 刘潇, 等. 盆底MRI在女性压力性尿失禁诊疗中的应用价值[J]. 中华放射学杂志, 2020, 54(4): 345-349.
[13] Li N, Cui C, Cheng Y, et al. Association between Magnetic Resonance Imaging Findings of the Pelvic Floor and de novo Stress Urinary Incontinence after Vaginal Delivery[J]. Korean J Radiol, 2018, 19(4): 715-723.
[14] Yaşar L, Telci SO, Doǧan K, et al. Predictive role of measurement of pelvic floor muscle thickness with static MRI in stress and mixed urinary incontinence[J]. Int Urogynecol J, 2019, 30(2): 271-277. http://pubmed.ncbi.nlm.nih.gov/29779185/
[15] 栗敏, 白玫, 韩悦. 女性压力性尿失禁盆隔裂孔径线变化的MRI研究[J]. 中华放射学杂志, 2015, 49(9): 661-664.
[16] Singh K, Reid WM, Berger LA. Magnetic resonance imaging of normal levator ani anatomy and function[J]. Obstet Gynecol, 2002, 99(3): 433-438. http://europepmc.org/abstract/med/11864670
[17] Xiao T, Chen Y, Gan Y, et al. Can Stress Urinary Incontinence Be Predicted by Ultrasound?[J]. AJR Am J Roentgenol, 2019, 213(5): 1163-1169.
[18] Ajay D, Kahokehr AA, Lentz AC, et al. Valsalva leak point pressure(VLPP)greater than 70 cm H2O is an indicator for sling success: a success prediction model for the male transobturator sling[J]. Int Urol Nephrol, 2022, 54(7): 1499-1503. doi: 10.1007/s11255-022-03222-4
[19] Rosier PF, Gajewski JB, Sand PK, et al. Executive summary: The International Consultation on Incontinence 2008——Committee on: "Dynamic Testing"; for urinary incontinence and for fecal incontinence. Part 1: Innovations in urodynamic techniques and urodynamic testing for signs and symptoms of urinary incontinence in female patients[J]. Neurourol Urodyn, 2010, 29(1): 140-145. http://www.sciencedirect.com/science/article/pii/S1569905610606835
[20] 黄健. 中国泌尿外科和男科疾病诊断治疗指南(2019版)[M]. 北京: 科学出版社, 2020: 350.
-

图(4)
表(6)
计量
- 文章访问数: 1012
- PDF下载数: 141
- 施引文献: 0