
Modular and progressive teaching strategy applied in training of robotic assisted radical prostatectomy
-
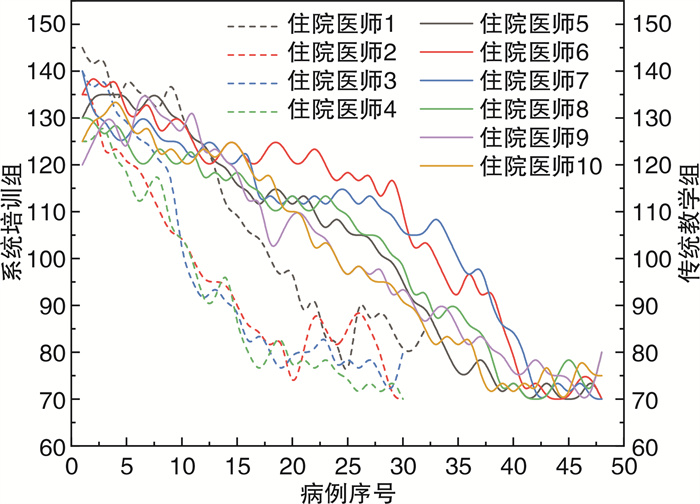
摘要: 目的 探索模块化进阶式教学法在机器人手术培训中的应用。方法 培训对象为4名完成住院总的住院医师,将手术按照难易程度分为5个模块,逐级培训。观察分析完成每个模块的病例数、手术的输血率、并发症发生率、手术时间、切缘阳性率。结果 4名住院医师顺利完成培训。他们需要52~57例的手术操作才能合格,平均手术时间为(94.62±12.40) min,平均输血率(2.29±0.94)%,平均并发症发生率(4.58±1.11)%。与全程由指导医师完成的手术相比,住院医师参与的手术的手术时间、输血率、并发症发生率、切缘阳性率无显著差异。与传统教学相比,系统培训学习曲线明显缩短。结论 模块化进阶式教学发在机器人手术培训中安全、可行,值得推广。Abstract: Objective To develop a modular and progressive teaching strategy applied in robotic surgery training.Methods The technique of robotic assisted radical prostatectomy (RARP) was divided into 5 modules of different complexities. Four residents participated in the study. Cases, blood transfusion rate, complications, operation time and positive surgical margin were analyzed.Results Four residents finished training. They required 52-57 cases until they were considered to be competent. Mean operation time was (94.62±12.40)min, transfusion rate is (2.29±0.94)%, complication rate was (4.58±1.11)%. There was no significant difference between the operations that residents participated and those the mentor performed alone. Compared with traditional teaching, systematic training can shorten the learning curve.Conculsion The modular and progressive teaching strategy is safe and feasible, and is worth being popularized.
-
Key words:
- robotic surgery /
- resident /
- radical prostatectomy /
- surgical teaching
-

-
表 1 术中表现评估表
熟练程度 1 2 3 4 5 机械臂的操控 深度 □ □ □ □ □准确操控器械到目标位置 力量 □ □ □ □ □牵拉组织张力适中 切换 □ □ □ □ □能迅速切换机械臂 碰撞 □ □ □ □ □操作过程器械无碰撞 三臂 □ □ □ □ □合理运用三臂 双手灵敏度 □ □ □ □ □双手很好配合使用 自主性 □ □ □ □ □无指导下独立完成手术 手术流畅度 □ □ □ □ □自信、有效、安全、流畅  下载: 导出CSV
下载: 导出CSV
表 2 观察指标
指标 住院医师1 住院医师2 住院医师3 住院医师4 指导医师 主刀前相关培训例数 干性实验室 1 1 1 1 1 湿性实验室 1 1 1 1 1 腹腔镜手术 25 19 21 28 - RARP助手 210 215 206 210 - 主刀培训病例数 模块① 3 4 3 5 - 模块② 9 8 8 10 - 模块③ 11 9 9 10 - 模块④ 15 16 14 15 - 模块⑤ 18 17 18 17 - 共计 56 54 52 57 53 手术数据 年龄/岁 69.30±11.59 67.40±7.35 68.60±7.14 67.90±5.43 69.70±7.80 PSA/(ng·mL-1) 14.28±7.33 17.53±10.10 13.09±9.28 13.20±6.07 10.90±4.89 手术时间/min 92.21±10.25 95.11±12.04 90.55±11.21 100.23±13.54 88.76±9.67 输血/例(%) 1(1.79) 2(3.70) 1(1.92) 1(1.75) 2(3.77) 并发症/例(%) 2(3.57) 2(3.70) 3(5.77) 3(5.26) 2(3.77) 留置尿管/d 14 14 14 14 14 切缘 T2/例(%) 30 24 27 25 27 + 3(10.00) 3(12.50) 4(14.81) 4(16.00) 3(11.11) - 27(90.00) 21(87.50) 23(85.19) 21(84.00) 24(88.89) T3/例(%) 26 30 25 32 26 + 12(46.15) 14(46.67) 11(44.00) 15(46.88) 12(46.15) - 14(53.85) 16(53.33) 14(56.00) 17(53.12) 14(53.85)
下载: 导出CSV
-
[1] Lovegrove C, Novara G, Mottrie A, et al. Structured and Modular Training Pathway for Robot-assisted Radical Prostatectomy(RARP): Validation of the RARP Assessment Score and Learning Curve Assessment[J]. Eur Urol, 2016, 69(3): 526-535. doi: 10.1016/j.eururo.2015.10.048
[2] Volpe A, Ahmed K, Dasgupta P, et al. Pilot Validation Study of the European Association of Urology Robotic Training Curriculum[J]. Eur Urol, 2015, 68(2): 292-299. doi: 10.1016/j.eururo.2014.10.025
[3] Rashid HH, Leung YY, Rashid MJ, et al. Robotic surgical education: a systematic approach to training urology residents to perform robotic-assisted laparoscopic radical prostatectomy[J]. Urology, 2006, 68(1): 75-79. doi: 10.1016/j.urology.2006.01.057
[4] Pasticier G, Rietbergen JB, Guillonneau B, et al. Robotically assisted laparoscopic radical prostatectomy: feasibility study in men[J]. Eur Urol, 2001, 40(1): 70-74. doi: 10.1159/000049751
[5] Wang RS, Ambani SN. Robotic Surgery Training: Current Trends and Future Directions[J]. Urol Clin North Am, 2021, 48(1): 137-146. doi: 10.1016/j.ucl.2020.09.014
[6] Nik-Ahd F, Souders CP, Houman J, et al. Robotic Urologic Surgery: Trends in Food and Drug Administration-Reported Adverse Events Over the Last Decade[J]. J Endourol, 2019, 33(8): 649-654. doi: 10.1089/end.2018.0802
[7] Balbona J, Patel T. The Hidden Curriculum: Strategies for Preparing Residents for Practice[J]. Curr Urol Rep, 2020, 21(10): 39. doi: 10.1007/s11934-020-00992-1
[8] Carrion DM, Rodriguez-Socarrás ME, Mantica G, et al. Current status of urology surgical training in Europe: an ESRU-ESU-ESUT collaborative study[J]. World J Urol, 2020, 38(1): 239-246. doi: 10.1007/s00345-019-02763-1
[9] Steinberg PL, Merguerian PA, Bihrle W 3rd, et al. The cost of learning robotic-assisted prostatectomy[J]. Urology, 2008, 72(5): 1068-1072. doi: 10.1016/j.urology.2007.11.118
[10] Bravi CA, Tin A, Vertosick E, et al. The Impact of Experience on the Risk of Surgical Margins and Biochemical Recurrence after Robot-Assisted Radical Prostatectomy: A Learning Curve Study[J]. J Urol, 2019, 202(1): 108-113. doi: 10.1097/JU.0000000000000147
[11] Cimen HI, Atik YT, Gul D, et al. Serving as a bedside surgeon before performing robotic radical prostatectomy improves surgical outcomes[J]. Int Braz J Urol, 2019, 45(6): 1122-1128. doi: 10.1590/s1677-5538.ibju.2019.0330
[12] Goh AC, Goldfarb DW, Sander JC, et al. Global evaluative assessment of robotic skills: validation of a clinical assessment tool to measure robotic surgical skills[J]. J Urol, 2012, 187(1): 247-252. doi: 10.1016/j.juro.2011.09.032
[13] Collins JW, Wisz P. Training in robotic surgery, replicating the airline industry. How far have we come?[J]. World J Urol, 2020, 38(7): 1645-1651. doi: 10.1007/s00345-019-02976-4
[14] Schroeck FR, de Sousa CA, Kalman RA, et al. Trainees do not negatively impact the institutional learning curve for robotic prostatectomy as characterized by operative time, estimated blood loss, and positive surgical margin rate[J]. Urology, 2008, 71(4): 597-601 doi: 10.1016/j.urology.2007.12.023
-
图(1)
表(2)
计量
- 文章访问数: 776
- PDF下载数: 146
- 施引文献: 0