
Clinical evaluation in patients with non-muscle invasive urothelial cancer of bladder selected by the second transurethral resection of bladder tumor
-
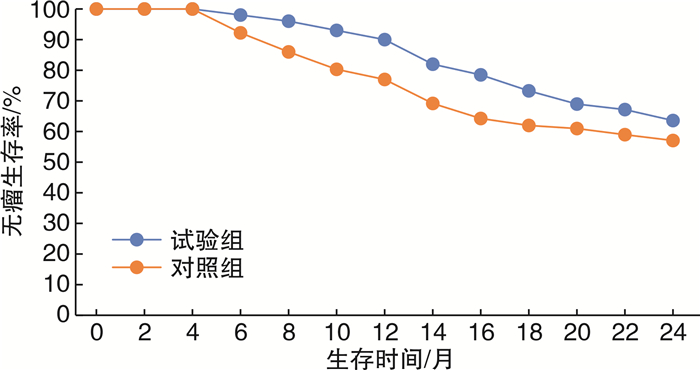
摘要: 目的 评价非肌层浸润性膀胱尿路上皮癌选择再次经尿道膀胱肿瘤电切术的临床疗效和应用价值。方法 2010年1月—2018年12月85例伴有高危因素膀胱癌患者,符合膀胱多发肿瘤(膀胱肿瘤同时发生2个及以上部位)、膀胱肿瘤CT或超声测定的最大径超过3 cm、T1G3期肿瘤、短期(3~6个月)复发肿瘤等条件之一的进入试验组。在施行初次经尿道膀胱肿瘤电切术(TURBt)后2~4周施行二次TURBt。与2004—2009年具有相同条件,行单次膀胱肿瘤经尿道电切术的76例高危膀胱癌患者(对照组)的治疗进行对照分析,应用单因素和多因素分析对试验组和对照组术后的复发和浸润进行预后性研究。结果 试验组85例和对照组76例全部随访,随访中位数28个月。试验组2年内高危膀胱肿瘤的复发率为36.3%,对照组为42.9%。试验组肿瘤肌层浸润率为20%,对照组为23.7%。试验组二次电切发现肿瘤残存20%,其中手术部位残存12%,其他部位8%;二次电切严重并发症9例(14.3%),其中膀胱穿孔4例,膀胱出血5例。两组膀胱浸润的35例患者中,其中16例行膀胱根治性切除手术(试验组8例,对照组8例),16例仍然选择保膀胱手术,3例选择非手术治疗。术后连续切片证明24例(68.6%)伴发膀胱原位癌。两组病理学分期、细胞分级差异无统计学意义(P>0.05),两组复发率比较差异有统计学意义(P< 0.05)。两组2年无瘤生存分析Kaplan-Meier氏法分析结果及log-rank检验差异有统计学意义(P< 0.05)。多因素分析显示膀胱原位癌和直径>3 cm肿瘤是选择再次电切术的危险因素。结论 再次电切提高了TURBt本身的质量,能有效区分残存肿瘤和早期复发肿瘤,但只能提供有限度的肿瘤病理分期和临床预后资料;对伴发原位癌不能准确分期,对广基最大径>3 cm肿瘤可能会降低临床实际分期,选择再次经尿道电切术应引起临床警示。Abstract: Objective To estimate the clinical significance and discussion on its clinical value of selecting second transurethral resection of bladder tumor(TURBt) in patients with non-muscle invasive bladder tumors.Methods From January 2010 to December 2018, of 85 patients with non-muscle invasive urothelial cancer of the bladder accompanied by high risk factors, including the multi-focal bladder tumors, bigger tumors of the max diameter over than 3 cm, T1G3 bladder tumors, and the recurrence bladder tumors within 3 to 6 months etcetera, entered into the study(the trail) in our hospital. They were performed by the second TURBt within 2 to 4 weeks following the initial resection, compared to 76 patients with the same risk factors(the control) only performed by the first TURBt from 2004 to 2009. The study observed on the status of the residual tumors after the initial resections and recurrence after the second resections. Statistical study was performed by univariate and multi-variate analysis in order to evaluate the prognosis of its recurrence and invasion.Results After a median of 28 months of follow-up, 85 in the trail and 76 in the control all had follow-up with the recurrence rate in 36.3% and 42.9% respectively, accompanied by the invasion rate of 20% in the trial and 23.7% in the control. The overall residual disease rate after the first TURBt was 20% in the trial, and the residual rate of operative locations was 12%, with the others in 8%. The serious complications performed by the second TURBt were in 9(14.3%), with the bladder ruptures in 4 and the bladder bleedings in 5. Of 35 cases of disease progression, 16 patients underwent radical cystectomies, 16 selected partial cystectomies, and 3 without operations, in which 24 patients showed the carcinoma in situ in continuous pathological sections(68.6%). There was no significance of tumor stage and cell grade between in the trial and in the control(P>0.05), but was a positive statistics in the recurrence rate each other(P< 0.05). It was a significant that the two years survival rate of tumor-free was analyzed by Kaplan-Meier's method and log-rank test between the trial and the control. The multivariate analysis showed that the carcinoma in situ and tumor size over 3 cm were the risk factors in patients with selecting second TURBt.Conclusion The second TURBt could improve the quality itself and differentiate the recurrence tumors or the residual tumors, but it only supplied the limited information in stage and prognosis of tumors. The second TURBt could not show the correct stage in patients with carcinoma in situ and understage in patients with tumor size over 3 cm.
-

-
表 1 试验组与对照组临床资料比较
例 组别 试验组(n=85) 对照组(n=76) P值 男/女 70/15 63/13 > 0.05 平均年龄/岁 67±5 64±4 > 0.05 肿瘤最大径/cm 3.3±0.3 3.1±0.2 > 0.05 单发/多发 52/33 46/30 > 0.05 有蒂/无蒂 43/42 38/38 > 0.05 肿瘤部位 三角区 24 22 > 0.05 后壁 15 22 > 0.05 侧避 18 21 > 0.05 顶壁 13 4 > 0.05 前壁 13 7 > 0.05 颈部(前列腺) 2 0 > 0.05 病理分期 > 0.05 pTa 35 21 pT1 50 55 细胞分级 > 0.05 Ⅰ 4 5 Ⅱ 41 33 Ⅲ 40 38 2年复发率/% 36.3 42.9 < 0.05 肌层浸润率/% 20.0(17/85) 23.7(18/76) > 0.05  下载: 导出CSV
下载: 导出CSV
表 2 logistic回归分析参数
变量 回归系数 标准误 比值比 95%可信区间 P值 原位癌 -2.674 0.893 0.883 0.334~2.986 0.024 肿瘤最大径 > 3 cm 1.679 0.643 3.022 1.032~5.097 0.033
下载: 导出CSV
-
[1] Ritch CR, Clark PE, Morgan TM. Restaging transurethral resection for non-muscle invasive bladder cancer: who, why, when, and how?[J]. Urol Clin North Am, 2013, 40(2): 295-304. doi: 10.1016/j.ucl.2013.01.009
[2] Babjuk M, Oosterlinck W, Sylvester R, et al. EAU guideline on nonmuscle-invasive urothelial carcinoma of the bladder, 2011 update[J]. Eur Urol, 2011, 59: 997-1008. doi: 10.1016/j.eururo.2011.03.017
[3] Gendy R, Delprado W, Brenner P, et al. Repeat transurethral resection for non-muscle-invasive bladder cancer: a contemporary series[J]. BJU Int, 2016, 117 Suppl 4: 54-59.
[4] 孙晓文, 燕东亮, 夏术阶, 等. 高危非浸润膀胱尿路上皮癌术后再活检和电切的临床意义[J]. 中华泌尿外科杂志, 2009, 30(4): 248-250. doi: 10.3760/cma.j.issn.1000-6702.2009.04.013
[5] Ramírez-Backhaus M, Domínguez-Escrig J, Collado A, et al. Restaging transurethral resection of bladder tumor for high-risk stage Ta and T1 bladder cancer[J]. Curr Urol Rep, 2012, 13(2): 109-114. doi: 10.1007/s11934-012-0234-4
[6] Schraml J, Silva J, Babjuk M. Current concept of transurethral resection of bladder cancer: from re-transurethral resection of bladder cancer to en-bloc resection[J]. Curr Opin Urol, 2018, 28(6): 591-597. doi: 10.1097/MOU.0000000000000542
[7] 陈锦超, 李腾, 宁向辉, 等. 二次电切阳性发现在T1期膀胱癌中的临床意义[J]. 中华医学杂志, 2016, 96(14): 1124-1127. doi: 10.3760/cma.j.issn.0376-2491.2016.14.013
[8] Cumberbatch M, Foerster B, Catto J, et al. Repeat Transurethral Resection in Non-muscle-invasive Bladder Cancer: A Systematic Review[J]. Eur Urol, 2018, 73(6): 925-933. doi: 10.1016/j.eururo.2018.02.014
[9] Krajewski W, Nowak Ł, Poletajew S, et al. The Impact of Restaging Transurethral Resection of Bladder Tumor on Survival Parameters in T1 Nonmuscle-Invasive Bladder Cancer: Systematic Review and Meta-Analysis[J]. J Endourol, 2020, 34(8): 795-804. doi: 10.1089/end.2020.0301
[10] Kukreja JB, Porten S, Golla V, et al. Absence of Tumor on Repeat Transurethral Resection of Bladder Tumor Does Not Predict Final Pathologic T0 Stage in Bladder Cancer Treated with Radical Cystectomy[J]. Eur Urol Focus, 2018, 4(5): 720-724. doi: 10.1016/j.euf.2016.12.005
[11] Deǧer MD, Çelik S, Yıldız A, et al. Can we perform frozen section instead of repeat transurethral resection in bladder cancer?[J]. Urol Oncol, 2021, 39(4): 237-239.
[12] Akand M, Muilwijk T, Raskin Y, et al. Quality Control Indicators for Transurethral Resection of Non-Muscle-Invasive Bladder Cancer[J]. Clin Genitourin Cancer, 2019, 17(4): e784-e792. doi: 10.1016/j.clgc.2019.04.014
[13] Hassan O, Murati Amador B, Lombardo KA, et al. Clinical significance of urothelial carcinoma ambiguous for muscularis propria invasion on initial transurethral resection of bladder tumor[J]. World J Urol, 2020, 38(2): 389-395. doi: 10.1007/s00345-019-02782-y
[14] 蒋书算, 曹健, 韩惟青, 等. 非肌层浸润性膀胱癌首次电切术后肿瘤残余及二次电切术后复发相关因素分析[J]. 临床泌尿外科杂志, 2021, 36(4): 264-269. https://www.cnki.com.cn/Article/CJFDTOTAL-LCMW202104003.htm
[15] Czech AK, Gronostaj K, Frydrych J, et al. Identification of potential prognostic factors for absence of residual disease in the second resection of T1 bladder cancer[J]. Cent European J Urol, 2019, 72(3): 252-257.
-
图(1)
表(2)
计量
- 文章访问数: 1997
- PDF下载数: 814
- 施引文献: 0