
Analysis of the application of the ARVUS technique in patients with oligometastatic prostate cancer during robot assisted prostatectomy
-
摘要: 目的 在接受机器人辅助前列腺切除术的寡转移患者中比较膀胱尿道重建支持(ARVUS) 技术及传统后加固技术的控尿功能恢复差异。方法 回顾性统计了54例接受机器人辅助前列腺癌切除术的寡转移前列腺癌患者,其中21例患者接受了ARVUS技术,33例患者接受了传统的后加固技术。记录两组患者的年龄、BMI、诊断时PSA、术前PSA、术前IPSS评分、病理指标、手术时长、术中及术后并发症。使用ICIQ-SF量表客观记录患者尿控情况,对比两组人群拔除尿管后1、3、6和12个月时的控尿功能差异。结果 ARVUS组和传统组拔除尿管后1个月的ICIQ-SF评分分别为9.85和11.42(P=0.04),3个月的评分分别为7.91和9.22(P=0.081),6个月的评分分别为4.76和6.42(P=0.047),12个月的评分分别为3.58和4.49(P=0.185)。根据Clavien-Dindo并发症分级,ARVUS组发生了1例1级并发症,2例2级并发症;传统组发生了2例1级并发症,2例2级并发症。暂未观察到吻合口漏尿、会阴部疼痛、尿道狭窄等并发症。结论 ARVUS技术用于寡转移前列腺癌的前列腺切除术中可改进患者半年内的控尿恢复速度。
-
关键词:
- 寡转移前列腺癌 /
- 前列腺切除术 /
- 控尿功能 /
- 膀胱尿道重建支持技术
Abstract: Objective To determine whether the ARVUS technique improves urinary continence after robotic-assisted radical prostatectomy for oligometastatic prostate cancer.Methods Fifty four patients with oligometastatic prostate cancer who underwent robot assisted prostatectomy were retrospectively analyzed. Among which, 21 patients received ARVUS technique and 33 patients received traditional posterior reconstruction(Rocco stitch). The age, BMI, PSA at diagnosis, preoperative PSA, preoperative IPSS score, pathology, operation duration, intraoperative and postoperative complications of the two groups were recorded. ICIQ-SF scale was used to objectively record the urinary continence of the patients, and the difference between the two groups at 1 month, 3 months, 6 months and 12 months after the removal of the catheter was compared.Results The ICIQ-SF scores of the ARVUS group and the control group were 9.85 and 11.42(P=0.04) at 1 month, 7.91 and 9.22(P=0.081) at 3 months, 4.76 and 6.42(P=0.047) at 6 months, and 3.58 and 4.49(P=0.185) at 12 months, respectively. According to Clavien Dindo complication classification, 1 case of grade 1 complication and 2 cases of grade 2 complication occurred in the ARVUS group; There were 2 grade 1 complications and 2 grade 2 complications in the traditional group. No anastomotic leakage, perineal pain and urethral stricture were observed.Conclusion The ARVUS technique may improve the early urinary continence in patients with oligometastatic prostate cancer after prostatectomy. -

-
表 1 两组患者基本情况比较
M(P25,P75),例(%) 项目 ARVUS组(21例) 传统组(33例) P值 年龄/岁 71(63,79) 67(53,80) 0.065 初诊时PSA/(ng·mL-1) 48(6,350) 56(16,277) 0.550 术前PSA/(ng·mL-1) 1.07(0.02,4.5) 0.62(0.04,3.6) 0.150 BMI/(kg·m-2) 22.6(18.3,28.1) 22.3(17.8,26.8) 0.560 IPSS评分/分 5.8(1,13) 5.5(0,15) 0.210 手术时间/min 124(93,181) 119(95,166) 0.400 病理侵犯状态 切缘阳性 6(28.6) 8(24.2) 0.720 尿道侵犯 2(9.5) 2(6.1) 0.640 膀胱颈侵犯 3(14.3) 2(6.1) 0.310 盆壁侵犯 1(4.7) 3(9.1) 0.055 术后并发症分级(Clavien-Dindo) 1级 1(4.7) 2(6.1) 0.960 2级 2(9.5) 2(6.1) 0.770 3级 0 0  下载: 导出CSV
下载: 导出CSV
-
[1] Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2018, 68(6): 394-424. doi: 10.3322/caac.21492
[2] Parker CC, James ND, Brawley CD, et al. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer(STAMPEDE): a randomised controlled phase 3 trial[J]. Lancet, 2018, 392(10162): 2353-2366. doi: 10.1016/S0140-6736(18)32486-3
[3] Boevé L, Hulshof M, Vis AN, et al. Effect on survival of androgen deprivation therapy alone compared to androgen deprivation therapy combined with concurrent radiation therapy to the prostate in patients with primary bone metastatic prostate cancer in a prospective randomised clinical trial: Data from the HORRAD Trial[J]. Eur Urol, 2019, 75(3): 410-418. doi: 10.1016/j.eururo.2018.09.008
[4] 中国临床肿瘤学会指南工作委员会. 中国临床肿瘤学会(CSCO)前列腺癌诊疗指南2021[M]. 北京: 人民卫生出版社, 2021: 11.
[5] Lardas M, Grivas N, Debray TPA, et al. Patient-and tumour-related prognostic factors for urinary incontinence after radical prostatectomy for nonmetastatic prostate cancer: a systematic review and meta-analysis[J]. Euro Urol Focus, 2021, 2021(4): 020.
[6] Tienza A, Robles JE, Hevia M, et al. Prevalence analysis of urinary incontinence after radical prostatectomy and influential preoperative factors in a single institution[J]. Aging Male, 2018, 21(1): 24-30. doi: 10.1080/13685538.2017.1369944
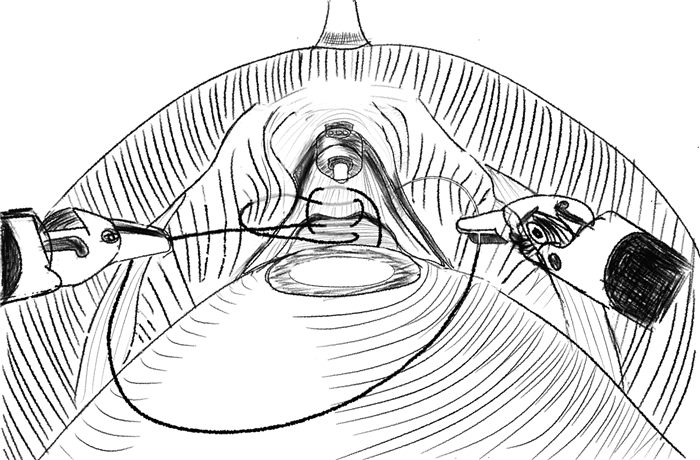
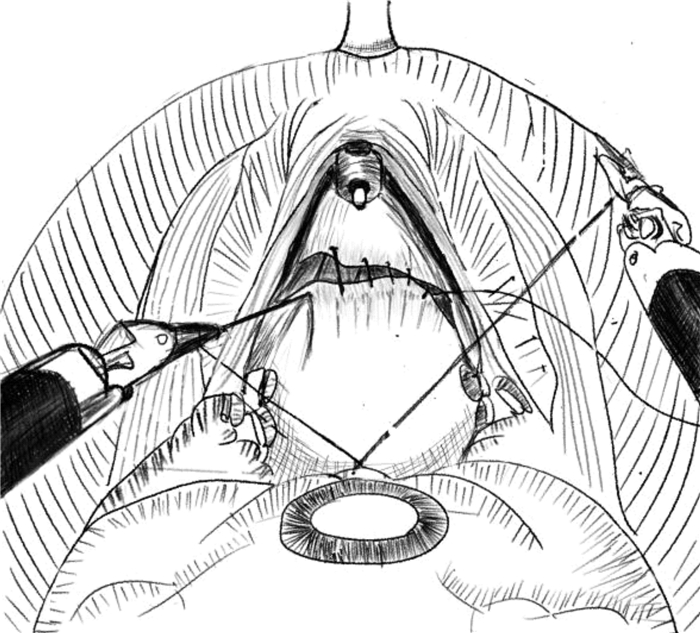
[7] Student V Jr, Vidlar A, Grepl M, et al. Advanced Reconstruction of Vesicourethral Support(ARVUS)during Robot-assisted Radical Prostatectomy: One-year Functional Outcomes in a Two-group Randomised Controlled Trial[J]. Eur Urol, 2017, 71(5): 822-830. doi: 10.1016/j.eururo.2016.05.032
[8] Rocco B, Gregori A, Stener S, et al. Posterior reconstruction of the rhabdosphincter allows a rapid recovery of continence after transperitoneal videolaparoscopic radical prostatectomy[J]. Eur Urol, 2007, 51(4): 996-1003. doi: 10.1016/j.eururo.2006.10.014
[9] Avery K, Donovan J, Peters TJ, et al. ICIQ: a brief and robust measure for evaluating the symptoms and impact of urinary incontinence[J]. Neurourol Urodyn, 2004, 23(4): 322-330. doi: 10.1002/nau.20041
[10] Dai B, Zhang S, Wan FN, et al. Combination of androgen deprivation therapy with radical local therapy versus androgen deprivation therapy alone for newly diagnosed oligometastatic prostate cancer: A Phase Ⅱ Randomized Controlled Trial[J]. Eur Urol Oncol, 2022, 5(5): 519-525. doi: 10.1016/j.euo.2022.06.001
[11] 程晓锋, 许嵩, 周晓晨, 等. 寡转移性PCa新辅助内分泌治疗后RARP与仅行RARP的短期临床疗效对比[J]. 临床泌尿外科杂志, 2021, 36(8): 627-632. doi: 10.13201/j.issn.1001-1420.2021.08.008
[12] Shin TY, Lee YS. Robot-assisted radical prostatectomy in the treatment of patients with clinically high-risk localized and locally advanced prostate cancer: single surgeons functional and oncologic outcomes[J]. BMC Urol, 2022, 22(1): 49. doi: 10.1186/s12894-022-00998-6
[13] Nyarangi-Dix JN, Görtz M, Gradinarov G, et al. Retzius-sparing robot-assisted laparoscopic radical prostatectomy: functional and early oncologic results in aggressive and locally advanced prostate cancer[J]. BMC Urol, 2019, 19(1): 113. doi: 10.1186/s12894-019-0550-9
[14] McCormick BZ, Chery L, Chapin BF. Contemporary outcomes following robotic prostatectomy for locally advanced and metastatic prostate cancer[J]. Transl Androl Urol, 2021, 10(5): 2178-2187. doi: 10.21037/tau-20-1002
[15] Abdollah F, Dalela D, Sood A, et al. Functional outcomes of clinically high-risk prostate cancer patients treated with robot-assisted radical prostatectomy: a multi-institutional analysis[J]. Prostate Cancer Prostatic Dis, 2017, 20(4): 395-400. doi: 10.1038/pcan.2017.26
[16] Nyarangi-Dix JN, Tosev G, Damgov I, et al. Recovery of pad-free continence in elderly men does not differ from younger men undergoing robot-assisted radical prostatectomy for aggressive prostate cancer[J]. World J Urol, 2020, 38(2): 351-360. doi: 10.1007/s00345-019-02797-5
[17] Kaul S, Savera A, Badani K, et al. Functional outcomes and oncological efficacy of Vattikuti Institute prostatectomy with Veil of Aphrodite nerve-sparing: an analysis of 154 consecutive patients[J]. BJU Int, 2006, 97(3): 467-472. doi: 10.1111/j.1464-410X.2006.05990.x
[18] Rosenberg JE, Jung JH, Edgerton Z, et al. Retzius-sparing versus standard robotic-assisted laparoscopic prostatectomy for the treatment of clinically localized prostate cancer[J]. Cochrane Database Syst Rev, 2020, 8: CD013641.
[19] Dal Moro F, Vladimir Student Jr., Ales Vidlar, et al. Advanced Reconstruction of Vesicourethral Support(ARVUS)during robot-assisted radical prostatectomy: one-year functional outcomes in a two-group randomised controlled trial[J]. Eur Urol, 2017, 71: 822-830. doi: 10.1016/j.eururo.2016.05.032
-
图(2)
表(1)
计量
- 文章访问数: 1166
- PDF下载数: 376
- 施引文献: 0