
Application of enhanced recovery after surgery in pediatric urology: a single-center 3-year experience
-
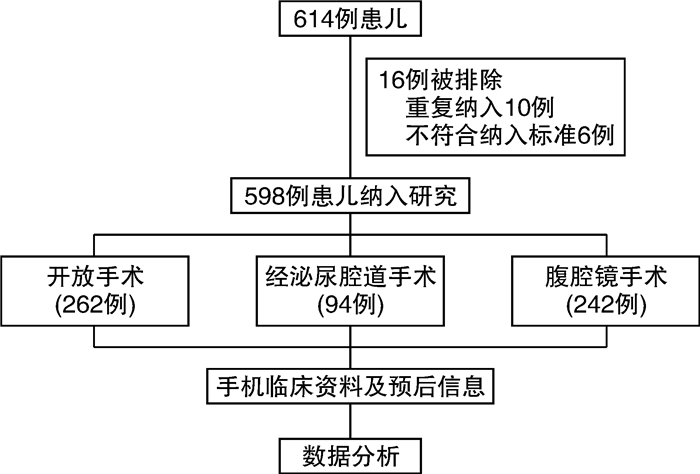
摘要: 目的 总结近3年中山大学附属第六医院泌尿外科手术患儿中应用加速康复外科的经验。方法 从医院病案系统收集2018年7月—2021年12月就诊于我科的614例患儿的病例资料,依据纳排标准,最终598例患儿纳入后续研究。收集这些患儿的一般临床资料和ERAS相关资料,包括住院费用、药物费用、手术方式、手术时间、术后住院时间、术后24 h出院率及30 d内再入院率等。结果 患儿的中位就诊年龄为5岁,其中97.8%的患儿在青春发育期前(< 12岁)就诊,男547例,女51例,开放手术262例,经泌尿腔道手术94例,腹腔镜手术242例,三、四级手术占比达85.4%。平均住院总费用为(1.52±0.88)万元,平均药物费用为(0.12±0.12)万元,占比约7.9%。平均手术时间为(99±81) min,平均术后住院时间为(1.2±1.5) d,术后24 h出院率达63.4%,而术后30 d内再入院率仅1.7%。结论 加速康复外科非选择性应用于泌尿外科手术患儿的围手术期管理是安全可行的,有助于患儿的术后恢复。Abstract: Objective To summarize the experience of applying enhanced recovery after surgery (ERAS) in children undergoing urological surgery in the Sixth Affiliated Hospital of Sun Yat-sen University in the past three years.Methods The data of 614 children who were treated in our department from July 2018 to December 2021 were collected from the hospital medical record system. According to the inclusion and exclusion criteria, 598 children were finally included in the follow-up study. The general clinical data and ERAS-related data of these children were collected, including hospitalization costs, drug costs, surgical methods, operation time, postoperative hospital stay, 24-hour discharge rate, and 30-day re-hospitalization rate.Results The median age of the children was 5 years old, and 97.8 % of the children visited the doctor before puberty (< 12 years old), including 547 males and 51 females. There were 262 cases of open surgery, 94 cases of urinary tract surgery, and 242 cases of laparoscopic surgery. The proportion of third and fourth-grade surgery was 85.4 %. The average total hospitalization cost was (15.2±8.8) thousand yuan, and the average drug cost was (1.2±1.2) thousand yuan, accounting for about 7.9 %. The average operation time was (99±81) min, the average postoperative hospital stay was (1.2±1.5) d, the discharge rate within 24 h after operation was 63.4 %, and the readmission rate within 30 d after operation was only 1.7 %.Conclusion Non-selective application of ERAS in perioperative management of children undergoing urological surgery is safe and feasible, so it's helpful for postoperative recovery of children.
-
Key words:
- enhanced recovery after surgery /
- pediatric urology /
- single center /
- experience summary
-

-
表 1 泌尿外科患儿ERAS-MDT围术期管理流程
处理措施 具体内容 术前 术前宣教 ①告知手术和麻醉过程,减轻家长精神压力、获取配合;②告知饮食要求和术后康复的详细步骤;③告知预设的出院标准及随访安排。 入院评估 营养状况评估,纠正贫血及低蛋白血症。再次评估营养状况。 控制感染 术前排除尿路感染、上呼吸道感染等。如存在感染,则感染控制后再进行手术。 肠道准备 不采取清洁灌肠;禁止机械性肠道准备;正常饮食至禁食;1岁以下婴幼儿单纯用开塞露通便1次。 术前饮食 固体进食至术前8 h;母乳进食至术前4 h;清饮至术前2 h(电解质或5%糖水5 mL/kg;1岁以下清饮为饮水)。 超前镇痛 术前晚8点口服非甾体类解热镇痛药(美林5~10 mg/kg)。 抗生素使用 术前30 min应用;如手术时间 > 3 h,可在术中重复1次。 术中 麻醉方案 依手术方式选择气管插管全麻或静脉全麻。诱导:丙泊酚2.5 mg/kg,芬太尼5 μg/kg,顺阿曲库铵0.2 mg/kg,地塞米松2 mg。麻醉维持:七氟醚3.5%,瑞芬太尼0.15 μg·kg-1·min-1,手术结束前30 min给予右美托咪定5 μg加入生理盐水泵注。 多模式镇痛 骶麻:0.1%~0.2%罗派卡因0.5~1.0 mL/kg;伤口局部浸润麻醉,静注凯纷。 液体管理 主要补充生理需要量按4 mL·kg-1·h-1计算,根据患儿心率、血压、尿量进行调整。 体温保护 设定适宜的术间温湿度,用充气加温设备预热手术床,术中避免不必要的暴露,对冲洗液及血制品进行加温,使术中患儿体温不低于36.0℃,术后及时盖好棉被。 手术方式 尽量选择微创的手术方式。 管道管理 除非必要,减少尿管的留置(常规术后第1天拔除),不放置鼻胃管与腹腔引流管。 伤口缝合 可吸收线美容缝合或皮肤胶水,无需拆线。 术后 术后镇痛 以NSAIDs为基础用药(美林5~10 mg/kg),不使用阿片类药物镇痛。 术后活动 术后清醒无不适即可下床活动,婴幼儿术后即可抱行。术后活动包括:①坐在床边或床外短时间活动(婴儿);②在病房内短暂步行或在床外喂食;③被父母抱行。 术后饮食 术后清醒后可适量饮水,无呛咳,可进流质饮食。母乳喂养者患儿术后自然哺乳。定时评估患儿进食后有无腹胀,有无哭闹,听肠鸣音,确保患儿进食后肠功能安全恢复。 术后抗感染 术后静脉用抗生素1 d,改用口服抗生素。 出院标准 恢复半流质饮食、口服止痛药效果良好、恢复适当活动。  下载: 导出CSV
下载: 导出CSV
表 2 598例手术患儿临床资料汇总
例(%),X±S,M(P25,P75) 临床资料 数值 年龄/岁 5(2,9) 婴儿期(≤1岁) 88(14.7) 幼儿期(2~3岁) 123(20.5) 学龄前期(4~7岁) 187(31.3) 学龄期(8~12岁) 187(31.3) 青春期(13~14岁) 13(2.2) 性别 男 547(91.5) 女 51(8.5) 体重/kg 19.6(13.5,30.9) 身高/cm 113(92,135) BMI 16.1(14.9,18.3) 费用/万元 住院总费用 1.52±0.88 药物费用 0.12±0.12 手术分级 一级手术 62(10.4) 二级手术 25(4.2) 三级手术 426(71.2) 四级手术 85(14.2) 手术方式 开放手术 262(43.8) 经泌尿腔道手术 94(15.7) 腹腔镜手术 242(40.5) 手术时间/min 99±81 术后住院时间/d 1.2±1.5 术后24 h出院 383(64.0) 术后30 d再入院 10(1.7)
下载: 导出CSV
表 3 开放手术患儿结果汇总
例(%),X±S,M(P25,P75) 手术名称 例数 年龄/岁 住院费用/万元 药物费用/万元 手术时间/min 术后住院时间/d 术后24 h出院 术后30 d再入院 阴茎整形术 170 8(6,10) 1.03±0.19 0.08±0.02 67±23 0.48±0.48 154(90.6) 1(0.4) 尿道下裂尿道成形 85 4(2,6) 1.80±0.42 0.14±0.07 134±46 2.82±1.35 5(6.0) 0(0) 其他开放手术 7 6(4.5,8.5) 1.41±1.41 0.12±0.11 90±122 1.25±1.81 5(71.4) 0(0)
下载: 导出CSV
表 4 经泌尿腔道手术患儿结果汇总
例(%),X±S,M(P25,P75) 手术名称 例数 年龄/岁 住院费用/万元 药物费用/万元 手术时间/min 术后住院时间/d 术后24 h出院 术后30 d再入院 膀胱镜检查/碎石 19 8(5.5,9) 1.79±1.49 0.29±0.23 45±41 1.39±0.86 4(21.1) 2(10.5) 输尿管双J管拔除 46 5(2.25,9) 0.52±0.28 0.08±0.09 12±62 0.57±0.44 38(82.6) 0(0) 其他腔内手术 29 5(2,8) 1.76±0.77 0.16±0.11 81±53 0.91±0.76 16(55.2) 3(10.3)
下载: 导出CSV
表 5 腹腔镜手术患儿结果汇总
例(%),X±S,M(P25,P75) 手术名称 例数 年龄/岁 住院费用/万元 药物费用/万元 手术时间/min 术后住院时间/d 术后24 h出院 术后30 d再入院 腹腔镜鞘状突高位结扎 68 3(2,5) 1.19±0.23 0.06±0.02 51±40 0.51±0.49 60(88.2) 0(0) 腹腔镜隐睾固定 101 2(1,5) 1.52±0.37 0.08±0.03 102±46 0.71±0.73 79(78.2) 1(1.0) 腹腔镜肾盂成形 41 6(2,9) 3.15±0.90 0.28±0.23 257±76 2.19±2.17 12(29.3) 2(4.9) 其他腹腔镜手术 32 5(3,8.25) 3.09±1.01 0.28±0.20 237±105 3.37±3.10 10(31.3) 1(3.1)
下载: 导出CSV
-
[1] Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation[J]. Br J Anaesth, 1997, 78(5): 606-617. doi: 10.1093/bja/78.5.606
[2] Ripollés-Melchor J, Ramírez-Rodríguez JM, Casans-Francés R, et al. Association Between Use of Enhanced Recovery After Surgery Protocol and Postoperative Complications in Colorectal Surgery: The Postoperative Outcomes Within Enhanced Recovery After Surgery Protocol(POWER)Study[J]. JAMA Surg, 2019, 154(8): 725-736. doi: 10.1001/jamasurg.2019.0995
[3] 唐维兵, 路长贵. 儿童加速康复外科的现状与展望[J]. 中华小儿外科杂志, 2019, 40(9): 769-771. doi: 10.3760/cma.j.issn.0253-3006.2019.09.001
[4] Dagorno C, Montalva L, Ali L, et al. Enhancing recovery after minimally invasive surgery in children: A systematic review of the literature and meta-analysis[J]. J Pediatr Surg, 2021, 56(12): 2157-2164. doi: 10.1016/j.jpedsurg.2021.04.004
[5] 黎介寿. 对Fast-track Surgery(快通道外科)内涵的认识[J]. 中华医学杂志, 2007, 87(8): 515-517. doi: 10.3760/j.issn:0376-2491.2007.08.004
[6] 朱维铭, 李宁, 黎介寿. 加速康复外科治疗[J]. 中国实用外科杂志2007, 27(1): 24-27. doi: 10.3321/j.issn:1005-2208.2007.01.007
[7] Song Y, Hu C, Yan P, et al. Effect of implementing enhanced recovery after surgery principles in the perioperative period of pediatric inguinal hernia[J]. Am J Transl Res, 2021, 13(5): 5540-5546.
[8] Arena S, Di Fabrizio D, Impellizzeri P, et al. Enhanced Recovery After Gastrointestinal Surgery(ERAS)in Pediatric Patients: a Systematic Review and Meta-analysis[J]. J Gastrointest Surg, 2021, 25(11): 2976-2988. doi: 10.1007/s11605-021-05053-7
[9] Tang J, Liu X, Ma T, et al. Application of enhanced recovery after surgery during the perioperative period in infants with Hirschsprung's disease-A multi-center randomized clinical trial[J]. Clin Nutr, 2020, 39(7): 2062-2069. doi: 10.1016/j.clnu.2019.10.001
[10] Lu J, Xue M, Fu P, et al. Evaluation of open reduction of distal humerus fractures in children after implementation of an enhanced recovery after surgery program[J]. BMC Musculoskelet Disord, 2022, 23(1): 705. doi: 10.1186/s12891-022-05675-1
[11] Rove KO, Strine AC, Wilcox DT, et al. Design and development of the Pediatric Urology Recovery After Surgery Endeavor(PURSUE)multicentre pilot and exploratory study[J]. BMJ Open, 2020, 10(11): e039035.
[12] Brindle ME, McDiarmid C, Short K, et al. Consensus Guidelines for Perioperative Care in Neonatal Intestinal Surgery: Enhanced Recovery After Surgery(ERAS®)Society Recommendations[J]. World J Surg, 2020, 44(8): 2482-2492. doi: 10.1007/s00268-020-05530-1
[13] McMullin JL, Hu QL, Merkow RP, et al. Are Kids More Than Just Little Adults? A Comparison of Surgical Outcomes[J]. J Surg Res, 2022, 279: 586-591. doi: 10.1016/j.jss.2022.06.012
[14] 褚元豪, 吴璇昭. 加速康复外科在小儿外科的临床应用[J]. 中国全科医学, 2021, 24(S2): 238-242. https://www.cnki.com.cn/Article/CJFDTOTAL-QKYX2021S2078.htm
[15] Azhar RA, Bochner B, Catto J, et al. Enhanced Recovery after Urological Surgery: A Contemporary Systematic Review of Outcomes, Key Elements, and Research Needs[J]. Eur Urol, 2016, 70(1): 176-187. doi: 10.1016/j.eururo.2016.02.051
[16] Haid B, Karl A, Koen M, et al. Enhanced Recovery after Surgery Protocol for Pediatric Urological Augmentation and Diversion Surgery Using Small Bowel[J]. J Urol, 2018, 200(5): 1100-1106. doi: 10.1016/j.juro.2018.06.011
[17] Short HL, Taylor N, Thakore M, et al. A survey of pediatric surgeons' practices with enhanced recovery after children's surgery[J]. J Pediatr Surg, 2018, 53(3): 418-430. doi: 10.1016/j.jpedsurg.2017.06.007
[18] Tanaka R, Lee SW, Kawai M, et al. Protocol for enhanced recovery after surgery improves short-term outcomes for patients with gastric cancer: a randomized clinical trial[J]. Gastric Cancer, 2017, 20(5): 861-871. doi: 10.1007/s10120-016-0686-1
[19] Rove KO, Edney JC, Brockel MA. Enhanced recovery after surgery in children: Promising, evidence-based multidisciplinary care[J]. Paediatr Anaesth, 2018, 28(6): 482-492. doi: 10.1111/pan.13380
[20] Crellin D, Harrison D, Santamaria N, et al. Comparison of the Psychometric Properties of the FLACC Scale, the MBPS and the Observer Applied Visual Analogue Scale Used to Assess Procedural Pain[J]. J Pain Res, 2021, 14: 881-892. doi: 10.2147/JPR.S267839
[21] Ekstein M, Weinbroum AA, Ben-Chaim J, et al. Comparison of Caudal Block vs. Penile Block vs. Intravenous Fentanyl Only in Children Undergoing Penile Surgery: A Prospective, Randomized, Double Blind Study[J]. Front Pediatr, 2021, 9: 654015. doi: 10.3389/fped.2021.654015
[22] Tao B, Liu K, Wang D, et al. Perioperative effects of caudal block on pediatric patients in laparoscopic upper urinary tract surgery: a randomized controlled trial[J]. BMC Pediatr, 2019, 19(1): 427. doi: 10.1186/s12887-019-1812-0
[23] Wiegele M, Marhofer P, Lönnqvist PA. Caudal epidural blocks in paediatric patients: a review and practical considerations[J]. Br J Anaesth, 2019, 122(4): 509-517. doi: 10.1016/j.bja.2018.11.030
[24] Wong YS, Pang KK, Tam YH. Hypospadias surgery in children: improved service model of enhanced recovery pathway and dedicated surgical team[J]. Hong Kong Med J, 2018, 24(3): 238-244.
[25] Rove KO, Brockel MA, Saltzman AF, et al. Prospective study of enhanced recovery after surgery protocol in children undergoing reconstructive operations[J]. J Pediatr Urol, 2018, 14(3): 252. e1-252. e9. doi: 10.1016/j.jpurol.2018.01.001
[26] 尧冰, 王德娟, 栗霞, 等. 泌尿外科患儿非选择性围手术期加速康复外科管理回顾性研究[J]. 中华小儿外科杂志, 2021, 42(9): 799-802. doi: 10.3760/cma.j.cn421158-20200329-00217
-
图(1)
表(5)
计量
- 文章访问数: 608
- PDF下载数: 261
- 施引文献: 0