
Clinical study on laparoscopic adrenalectomy via three-layered adrenal margin approach
-
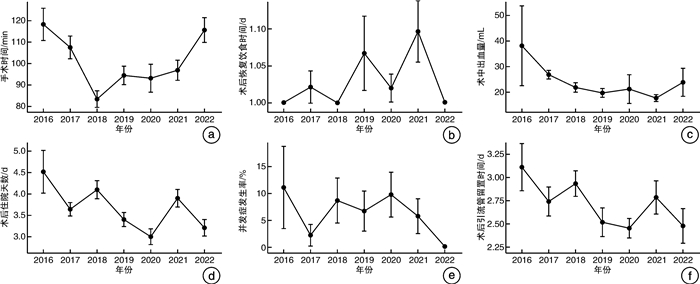
摘要: 目的 总结肾上腺边缘入路三层面后腹腔镜肾上腺手术在治疗全人群肾上腺疾病的临床疗效。方法 回顾性收集在福建省立医院施行肾上腺边缘入路三层面后腹腔镜肾上腺手术的302例患者的临床资料。手术步骤第一、第二层面与常规三层面技术相同,肾上腺边缘入路第三层面为肾周脂肪与肾上腺之间。按照2016—2017年、2018—2019年和2020—2022年进行分组,统计分析、比较3组间患者基本特征及围手术期数据。结果 所有患者均成功进行了后腹腔镜肾上腺手术,排除肿瘤大于6 cm的19例患者,本研究共纳入283患者,无中转开放手术,无非计划切除肾上腺。男119例,女164例;病变位于左侧173例,右侧110例。平均年龄为(44.84±12.22)岁,平均体重指数(BMI)为(23.82 ±3.23) kg/m2,平均肿瘤直径为(2.96±1.49) cm。3组间患者基本特征差异均无统计学意义(P>0.05)。2016—2017年组手术时间最长,2018—2019年组手术时间最短,平均手术时间为(98.26±36.95) min,3组间手术时间差异有统计学意义(P < 0.05)。平均术中出血量为(22.48±27.06) mL,平均引流管留置时间为(2.69±1.05) d,术后平均住院天数为(3.62±1.43) d。围手术期并发症发生率为6%,各组间差异无统计学意义。结论 肾上腺边缘入路三层面后腹腔镜肾上腺手术安全、可行、并发症少,无非计划切除同侧肾上腺。该技术有望成为肾上腺外科疾病的手术方法之一。
-
关键词:
- 腹腔镜 /
- 后腹腔镜肾上腺切除术 /
- 肾上腺 /
- 肾上腺边缘入路三层面 /
- 三层面
Abstract: Objective To provide a comprehensive summary of the clinical efficacy of laparoscopic adrenalectomy via three-layered adrenal margin approach for the treatment of adrenal diseases in the general population.Methods The clinical records of 302 patients who underwent laparoscopic adrenalectomy via three-layered adrenal margin approach were retrospectively examined. The first and second layers of surgical procedures are the same as the conventional three-layer techniques. The adrenal margin approach third layer was situated amidst the perirenal adipose tissue and adrenal gland. The patients were stratified into three groups based on the time periods of 2016—2017, 2018—2019, and 2020—2022, and their demographic characteristics and perioperative data were statistically analyzed and compared among these groups.Results Retro-laparoscopic adrenal surgery was successfully performed on all patients, except of 19 patients due to tumor diameter >6 cm. A total of 283 patients were included in this study without any conversions to open surgery or unplanned excisions of the adrenal glands. Among the patients, 119 were male and 164 were female, with an average age of (44.84±12.22) years old and BMI of (23.82±3.23) kg/m2. The lesions occurred on the left side in 173 cases and on the right side in 110 cases, with an average tumor diameter of (2.96±1.49) cm. There were no significant differences in basic characteristics observed among the three groups(P>0.05). The 2016—2017 group had the longest operation time, while the 2018—2019 group had the shortest. The average operation time was (98.26±36.95) minutes, and there was a statistically significant difference among the three groups(P < 0.05). The mean intraoperative blood loss was (22.48±27.06) mL, the mean duration of drainage was (2.69±1.05) days, and the mean length of postoperative hospital stay was (3.62±1.43) days. The incidence rate of perioperative complications was 6%, with no significant differences observed among all groups(P>0.05).Conclusion The laparoscopic adrenalectomy via three-layered adrenal margin approach is a safe and feasible method with less complications and without unplanned excisions of the adrenal glands. It is expected to become one of the preferred surgical methods for treating adrenal diseases. -

-
表 1 行肾上腺边缘入路三层面后腹腔镜肾上腺手术患者基本特征
例(%),X±S 项目 总体(283例) 2016—2017年组
(64例)2018—2019年组
(91例)2020—2022年组
(128例)χ2/F P值 性别 1.41 0.523 男 119(42.0) 31(48.4) 36(39.6) 52(40.6) 女 164(58.0) 33(51.6) 55(60.4) 76(59.4) 年龄/岁 44.84±12.22 47.25±12.20 47.52±12.32 50.54±12.02 2.51 0.083 肿瘤位置 1.51 0.571 右侧 110(38.9) 28(43.8) 37(40.7) 45(35.2) 左侧 173(61.1) 36(56.2) 54(59.3) 83(64.8) BMI/(kg/m2) 23.82±3.23 24.03±3.10 23.98±3.13 23.61±3.38 0.50 0.806 肿瘤直径/cm 2.96±1.49 3.13±1.44 2.87±1.25 2.94±1.67 0.56 0.446 ASA分级 46.60 < 0.001 Ⅰ 1(0.4) 0(0) 1(1.1) 0(0) Ⅱ 178(62.9) 52(81.3) 72(79.1) 54(42.2) Ⅲ 103(36.4) 12(18.7) 18(19.8) 73(57.0) Ⅳ 1(0.4) 0(0) 0(0) 1(0.8) 病理类型 1.81 0.870 肾上腺皮质腺瘤 208(73.5) 43(67.2) 69(75.8) 96(75.0) 嗜铬细胞瘤 29(10.2) 8(12.5) 8(8.8) 13(10.2) 其他肿瘤 46(16.3) 13(20.3) 14(15.4) 19(14.8)  下载: 导出CSV
下载: 导出CSV
表 2 行肾上腺边缘入路三层面后腹腔镜肾上腺手术患者围手术期数据比较
例(%),X±S 项目 总体(283例) 2016—2017年组
(64例)2018—2019年组
(91例)2020—2022年组
(128例)χ2/F P值 手术时间a)/min 98.26±36.95 110.58±35.90 88.73±28.64 98.88±40.84 6.88 0.002 术中出血量/mL 22.48±27.06 29.84±36.17 20.65±11.68 20.09±29.06 3.12 < 0.001 引流管留置时间/d 2.69±1.05 2.84±1.09 2.73±0.99 2.59±1.07 1.28 0.119 恢复饮食时间 5.06 0.374 术后第1天 274(96.8) 63(98.4) 89(97.8) 122(95.3) 术后第2天 8(2.8) 1(1.6) 1(1.1) 6(4.7) 术后第3天 1(0.4) 0(0) 1(1.1) 0(0) 并发症(Clavien-Dindo分级) 3.12 0.983 无 266(94.0) 61(95.3) 84(92.3) 121(94.5) Ⅰ 6(2.1) 1(1.6) 3(3.3) 2(1.6) Ⅱ 10(3.5) 2(3.1) 3(3.3) 5(3.9) Ⅲ 1(0.4) 0(0) 1(1.1) 0(0) 术后住院天数/d 3.62±1.43 3.88±1.52 3.75±1.36 3.40±1.42 2.94 0.010 非计划切除肾上腺b) 0(0) 0(0) 0(0) 0(0) - 注:a)手术时间:由于缺乏记录从手术开始到缝皮结束的时间,因此手术时间定义为麻醉系统记录的麻醉开始到麻醉结束时间;b)非计划切除肾上腺:定义为术前拟行保留正常肾上腺组织,但是因为肾上腺暴露不佳,术中完整切除肾上腺者。
下载: 导出CSV
-
[1] Munver R, Ilbeigi P. Retroperitoneal laparoscopic adrenalectomy[J]. Curr Urol Rep, 2005, 6(1): 72-77. doi: 10.1007/s11934-005-0070-x
[2] Raffaelli M, De Crea C, Bellantone R. Laparoscopic adrenalectomy[J]. Gland surgery, 2019, 8(Suppl 1): S41-S52.
[3] Zhang X, Fu B, Lang B, et al. Technique of anatomical retroperitoneoscopic adrenalectomy with report of 800 cases[J]. J Urol, 2007, 177(4): 1254-1257. doi: 10.1016/j.juro.2006.11.098
[4] Zhang X, Wang B, Ma X, et al. Laparoscopic adrenalectomy for beginners without open counterpart experience: initial results under staged training[J]. Urology, 2009, 73(5): 1061-1065. doi: 10.1016/j.urology.2008.11.058
[5] Kozłowski T, Choromanska B, Wojskowicz P, et al. Laparoscopic adrenalectomy: lateral transperitoneal versus posterior retroperitoneal approach-prospective randomized trial[J]. Wideochir Inne Tech Maloinwazyjne, 2019, 14(2): 160-169.
[6] Conzo G, Tartaglia E, Gambardella C, et al. Minimally invasive approach for adrenal lesions: Systematic review of laparoscopic versus retroperitoneoscopic adrenalectomy and assessment of risk factors for complications[J]. Int J Surg, 2016, 28 Suppl 1: S118-S123.
[7] Khene ZE, Peyronnet B, Mathieu R, et al. Analysis of the impact of adherent perirenal fat on peri-operative outcomes of robotic partial nephrectomy[J]. World J Urol, 2015, 33(11): 1801-1806. doi: 10.1007/s00345-015-1500-0
[8] Davidiuk AJ, Parker AS, Thomas CS, et al. Mayo adhesive probability score: an accurate image-based scoring system to predict adherent perinephric fat in partial nephrectomy[J]. Eur Urol, 2014, 66(6): 1165-1171. doi: 10.1016/j.eururo.2014.08.054
[9] Erbil Y, Barbaros U, Sari S, et al. The effect of retroperitoneal fat mass on surgical outcomes in patients performing laparoscopic adrenalectomy: the effect of fat tissue in adrenalectomy[J]. Surg Innov, 2010, 17(2): 114-119. doi: 10.1177/1553350610365703
[10] Hu M, Yang Z, Chen Y, et al. Modified three-level techniques of retroperitoneal laparoscopic procedures to treat adrenal lesions for patients with BMI ≥25 kg/m2[J]. Int J Med Sci, 2020, 17(18): 3107-3111. doi: 10.7150/ijms.49574
[11] Fan Y, Kong G, Meng Y, et al. Comparative assessment of surgeons' task performance and surgical ergonomics associated with conventional and modified flank positions: a simulation study[J]. Surg Endosc, 2014, 28(11): 3249-3256. doi: 10.1007/s00464-014-3598-3
[12] Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience[J]. Ann Surg, 2009, 250(2): 187-196. doi: 10.1097/SLA.0b013e3181b13ca2
[13] Yip L, Duh QY, Wachtel H, et al. American Association of Endocrine Surgeons Guidelines for Adrenalectomy: Executive Summary[J]. JAMA Surg, 2022, 157(10): 870-877. doi: 10.1001/jamasurg.2022.3544
[14] Hue JJ, Ahorukomeye P, Bingmer K, et al. A comparison of robotic and laparoscopic minimally invasive adrenalectomy for adrenal malignancies[J]. Surg Endosc, 2022, 36(7): 5374-5381. doi: 10.1007/s00464-021-08827-x
[15] 韩毅力, 赵佳晖, 罗勇, 等. 经腹腔和经腹膜后入路机器人辅助腹腔镜治疗巨大体积肾上腺肿瘤45例分析[J]. 现代泌尿外科杂志, 2023, 28(1): 46-49, 58. https://www.cnki.com.cn/Article/CJFDTOTAL-MNWK202301008.htm
[16] Pan XF, Wang L, Pan A. Epidemiology and determinants of obesity in China[J]. Lancet Diabetes Endocrinol, 2021, 9(6): 373-392. doi: 10.1016/S2213-8587(21)00045-0
[17] 吴侃, 张帆, 张富勋, 等. 经腹膜后途径与经腹腔途径腹腔镜肾上腺切除术治疗肾上腺皮质癌的疗效和安全性对比研究[J]. 中华泌尿外科杂志, 2022, 43(11): 830-834.
[18] 张二伟, 徐进松, 李冠儒, 等. 日间模式下的腹腔镜肾上腺肿瘤切除术的临床研究[J]. 临床泌尿外科杂志, 2022, 37(11): 866-868. http://lcmw.cbpt.cnki.net/WKC/WebPublication/paperDigest.aspx?paperID=f64c48d3-41fb-491c-8aff-b354e743b7e3
[19] 李慧, 卞晓洁, 叶定伟. 腹腔镜切除肾上腺醛固酮腺瘤的短期及长期随访研究[J]. 临床泌尿外科杂志, 2022, 37(3): 205-209. http://lcmw.cbpt.cnki.net/WKC/WebPublication/paperDigest.aspx?paperID=71ddc206-43f3-4d30-ada7-1e3b1961b1c4
[20] Kook Y, Choi HR, Kang SW, et al. Laparoscopic adrenalectomy: comparison of outcomes between posterior retroperitoneoscopic and transperitoneal adrenalectomy with 10 years' experience[J]. Gland Surg, 2021, 10(7): 2104-2112. doi: 10.21037/gs-21-178
[21] Limberg J, Stefanova D, Ullmann TM, et al. Not all laparoscopic adrenalectomies are equal: analysis of postoperative outcomes based on tumor functionality[J]. Surg Endosc, 2021, 35(6): 2601-2606. doi: 10.1007/s00464-020-07678-2
[22] Vatansever S, Nordenström E, Raffaelli M, et al. Robot-assisted versus conventional laparoscopic adrenalectomy: Results from the EUROCRINE Surgical Registry[J]. Surgery, 2022, 171(5): 1224-1230. doi: 10.1016/j.surg.2021.12.003
-

图(2)
表(2)
计量
- 文章访问数: 1056
- PDF下载数: 224
- 施引文献: 0