
Effect of surgical decision based on computed tomography on patients with unilateral aldosterone-producing adenoma
-
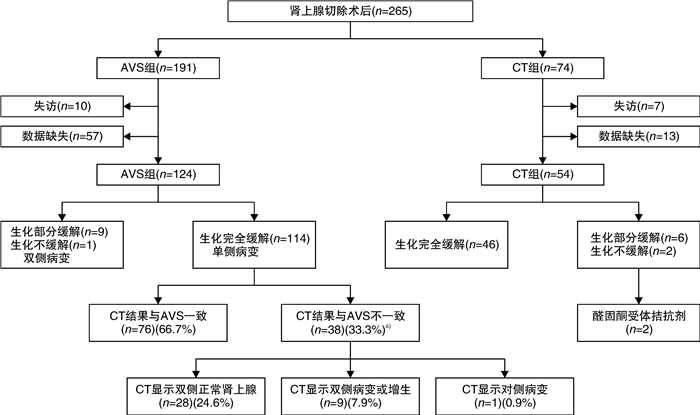
摘要: 目的 单侧肾上腺病变的原发性醛固酮增多症(primary aldosteronism,PA)可通过肾上腺切除术治愈或改善。目前指南推荐肾上腺静脉采血(adrenal venous sampling,AVS)作为诊断金标准。基于计算机断层扫描(CT)影像的手术决策仅被推荐用于年龄 < 35岁的单侧腺瘤患者。本研究旨在比较不同年龄组的单侧醛固酮腺瘤患者基于CT或AVS手术的疗效。方法 回顾性分析2018年6月—2021年1月在上海交通大学医学院附属瑞金医院因PA行单侧肾上腺切除术的178例患者的临床资料,根据决定手术的方式,分为CT组(54例)及AVS组(124例)。经过1年的随访,根据原发性醛固酮增多症手术结局(primary aldosteronism surgical outcome,PASO)标准评估术后临床和生化缓解率。结果 CT组与AVS组完全临床缓解率(46.3% vs 47.6%,P=0.875)和完全生化缓解率(88.8% vs 91.9%,P=0.515)比较,差异均无统计学意义。结论 这项研究表明,基于CT影像决策的手术可能适用于年龄范围更广的单侧醛固酮腺瘤患者。而对于双侧肾上腺正常或双侧肾上腺病变的PA患者,AVS仍是必需的诊断标准。Abstract: Objective Primary aldosteronism(PA) with unilateral adrenal disease can be cured or improved by adrenalectomy. Guidelines recommend adrenal venous sampling(AVS) to identify patients for surgical management. Currently, surgeries based on computed tomography(CT) images are only recommended for PA patients aged < 35 years with visible unilateral adenoma. We aimed to compare the outcomes between CT-based surgery and AVS-based surgery for PA patients with visible unilateral adenoma among different age groups.Methods A cohort study of 178 PA patients who underwent unilateral adrenalectomy at Ruijin hospital between June 2018 and January 2021 was conducted. Patients were grouped retrospectively according to how surgical decisions were made, CT group(54 cases) and AVS group(124 cases). Clinical and biochemical outcomes were analyzed according to primary aldosteronism surgical outcome(PASO) criteria after 1 year follow-up.Results The complete clinical success(46.3% vs 47.6%, P=0.875) and complete biochemical success(88.8% vs 91.9%, P=0.515) were similar between CT group and AVS group.Conclusion Surgery based on CT images might be feasible for PA patients with visible unilateral adenoma, while for PA patients with normal adrenal or bilateral adrenal lesions, the right treatment strategy would be obtained by the AVS.
-
Key words:
- adrenalectomy /
- computed tomography /
- adrenal vein sampling /
- primary aldosteronism /
- surgical outcomes
-

-
表 1 患者基线数据及随访数据
例(%),X±S,M(Min,Max) 项目 全部(178例) 手术决策方式 P值 CT组(54例) AVS组(124例) 基线数据 年龄/岁 46±13 42±13 47±12 0.021 性别(女) 92(51.7) 34(63.0) 58(46.8) 0.034 BMI/(kg/m2) 24.9±4.3 25.2±4.0 24.8±4.6 0.687 醛固酮浓度/(pg/mL) 357.0(155.0,1170.0) 331.5(213.0,996.0) 387.5(155.0,1 170.0) 0.614 血浆肾素活性/(ng/mL/h) 0.16(0.01,2.23) 0.13(0.01,1.94) 0.17(0.01,2.23) 0.345 ARR 2 240.1(298.6,6 300.0) 3 156.4(362.4,6 300.0) 2 074.4(298.6,5 850.0) 0.073 血钾浓度/mmol/L 2.71±0.47 2.70±0.49 2.72±0.47 0.819 病灶直径/mm 13.5±5.4 15.8±6.3 12.6±4.7 0.011 eGFR/(mL/min/1.73m2) 95.7±18.0 88.3±17.9 99.0±17.2 0.010 收缩压/mmHg 158±19 154±24 163±18 0.050 舒张压/mmHg 94±13 93±12 94±13 0.572 降压药服用剂量(DDD) 3.0(2.0,4.0) 3.0(2.0,5.0) 3.0(2.0,4.0) 0.369 随访数据 醛固酮浓度/(pg/mL) 87.0(30.0,367.0) 95.5(31.0,367.0) 81.5(30.0,330.0) 0.111 血浆肾素活性/(ng/mL/h) 1.11(0.05,7.90) 0.88(0.05,6.23) 1.23(0.12,7.90) 0.199 ARR>300 16(9.0) 6(11.1) 10(8.1) 0.632 血钾浓度/(mmol/L) 4.30±0.41 4.37±0.47 4.27±0.38 0.293 收缩压/mmHg 134±13 132±13 134±134 0.099 舒张压/mmHg 94±13 93±12 94±13 0.727 降压药服用剂量(DDD) 1.0(0.0,3.0) 1.0(0.0,3.0) 1.0(0.0,3.0) 0.645  下载: 导出CSV
下载: 导出CSV
表 2 术后临床及生化缓解
例(%) 指标 全部(178例) 手术决策方式 P值 CT(54例) AVS(124例) 临床缓解 完全缓解 84(47.2) 25(46.3) 59(47.6) 0.875 部分缓解 90(50.6) 27(50.0) 63(50.8) 0.921 不缓解 4(2.2) 2(3.7) 2(1.6) 0.388 生化缓解 完全缓解 162(91.0) 48(88.9) 114(91.9) 0.515 部分缓解 13(7.3) 4(7.4) 9(7.3) 0.972 不缓解 3(1.7) 2(3.7) 1(0.8) 0.169
下载: 导出CSV
表 3 不同年龄分层的临床及生化缓解率
例 年龄 临床缓解 生化缓解 全部 手术决策方式 P值 全部 手术决策方式 P值 CT组 AVS组 CT组 AVS组 ≤35岁(46例) 0.711 0.465 完全缓解 39 14/16 25/30 45 16/16 29/30 部分+不缓解 7 2/16 5/30 1 0/16 1/30 36~45岁(44例) 0.803 0.836 完全缓解 27 7/12 20/32 40 12/13 28/31 部分+不缓解 17 5/12 12/32 4 1/13 3/31 46~55岁(39例) 0.695 0.536 完全缓解 8 2/12 6/27 34 9/11 25/28 部分+不缓解 31 10/12 21/27 5 2/11 3/28 ≥56岁(49例) 0.506 0.220 完全缓解 10 2/14 8/35 43 11/14 32/35 部分+不缓解 39 12/14 27/35 6 3/14 3/35 6
下载: 导出CSV
表 4 影响手术效果因素分析
变量因素 临床缓解 生化缓解 OR(95%CI) P值 OR(95%CI) P值 年龄 0.949(0.880~0.987) 0.013 1.121(0.901~1.266) 0.302 血钾浓度 0.890(0.695~1.231) 0.129 1.275(0.642~2.372) 0.192 BMI 0.835(0.739~0.944) 0.014 0.955(0.944~0.982) 0.136 eGFR 1.009(0.981~1.038) 0.516 0.965(0.931~1.001) 0.055 性别(女) 1.051(0.434~2.543) 0.913 0.896(0.305~2.348) 0.748 病灶直径 1.040(0.946~1.144) 0.146 1.073(0.976~1.180) 0.415 术后ARR不缓解(参考:未发现) 5.184(1.948~13.799) 0.001 NA NA 手术决策方式(参考:CT影像) 0.907(0.334~2.467) 0.849 0.925(0.297~2.887) 0.894
下载: 导出CSV
-
[1] Rossi GP. Primary Aldosteronism: JACC State-of-the-Art Review[J]. J Am Coll Cardiol, 2019, 74(22): 2799-2811. doi: 10.1016/j.jacc.2019.09.057
[2] Funder JW, Carey RM, Mantero F, et al. The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline[J]. J Clin Endocrinol Metab, 2016, 101(5): 1889-1916. doi: 10.1210/jc.2015-4061
[3] Monticone S, D'Ascenzo F, Moretti C, et al. Cardiovascular events and target organ damage in primary aldosteronism compared with essential hypertension: a systematic review and meta-analysis[J]. Lancet Diabetes Endocrinol, 2018, 6(1): 41-50. doi: 10.1016/S2213-8587(17)30319-4
[4] Velema M, Dekkers T, Hermus A, et al. Quality of Life in Primary Aldosteronism: A Comparative Effectiveness Study of Adrenalectomy and Medical Treatment[J]. J Clin Endocrinol Metab, 2018, 103(1): 16-24. doi: 10.1210/jc.2017-01442
[5] Rossi GP, Auchus RJ, Brown M, et al. An expert consensus statement on use of adrenal vein sampling for the subtyping of primary aldosteronism[J]. Hypertension, 2014, 63(1): 151-160. doi: 10.1161/HYPERTENSIONAHA.113.02097
[6] Reincke M, Bancos I, Mulatero P, et al. Diagnosis and treatment of primary aldosteronism[J]. Lancet Diabetes Endocrinol, 2021, 9(12): 876-892. doi: 10.1016/S2213-8587(21)00210-2
[7] Deinum J, Prejbisz A, Lenders J, et al. Adrenal Vein Sampling Is the Preferred Methodsto Select Patients With Primary Aldosteronism for Adrenalectomy: Con Side of the Argument[J]. Hypertension, 2018, 71(1): 10-14. doi: 10.1161/HYPERTENSIONAHA.117.09294
[8] Lim V, Guo Q, Grant CS, et al. Accuracy of adrenal imaging and adrenal venous sampling in predicting surgical cure of primary aldosteronism[J]. J Clin Endocrinol Metab, 2014, 99(8): 2712-2719. doi: 10.1210/jc.2013-4146
[9] Rossi GP, Crimì F, Rossitto G, et al. Feasibility of Imaging-Guided Adrenalectomy in Young Patients With Primary Aldosteronism[J]. Hypertension, 2022, 79(1): 187-195. doi: 10.1161/HYPERTENSIONAHA.121.18284
[10] Dekkers T, Prejbisz A, Kool L, et al. Adrenal vein sampling versus CT scan to determine treatment in primary aldosteronism: an outcome-based randomised diagnostic trial[J]. Lancet Diabetes Endocrinol, 2016, 4(9): 739-746. doi: 10.1016/S2213-8587(16)30100-0
[11] Williams TA, Lenders J, Mulatero P, et al. Outcomes after adrenalectomy for unilateral primary aldosteronism: an international consensus on outcome measures and analysis of remission rates in an international cohort[J]. Lancet Diabetes Endocrinol, 2017, 5(9): 689-699. doi: 10.1016/S2213-8587(17)30135-3
[12] Dekkers T, ter Meer M, Lenders JW, et al. Adrenal nodularity and somatic mutations in primary aldosteronism: one node is the culprit?[J]. J Clin Endocrinol Metab, 2014, 99(7): E1341-E1351. doi: 10.1210/jc.2013-4255
[13] Vorselaars W, Nell S, Postma EL, et al. Clinical Outcomes After Unilateral Adrenalectomy for Primary Aldosteronism[J]. JAMA Surg, 2019, 154(4): e185842. doi: 10.1001/jamasurg.2018.5842
[14] Monticone S, Viola A, Rossato D, et al. Adrenal vein sampling in primary aldosteronism: towards a standardised protocol[J]. Lancet Diabetes Endocrinol, 2015, 3(4): 296-303. doi: 10.1016/S2213-8587(14)70069-5
[15] Ma D, Liu X, Zeng L, et al. The role of adrenal venous sampling and computed tomography in the management of primary aldosteronism[J]. J Hypertens, 2021, 39(2): 310-317. doi: 10.1097/HJH.0000000000002634
[16] Araujo-Castro M, Paja Fano M, González Boillos M, et al. Adrenal venous sampling in primary aldosteronism: Experience of a Spanish multicentric study(Results from the SPAIN-ALDO Register)[J]. Endocrine, 2022, 78(2): 363-372. doi: 10.1007/s12020-022-03122-8
[17] Williams TA, Burrello J, Sechi LA, et al. Computed Tomography and Adrenal Venous Sampling in the Diagnosis of Unilateral Primary Aldosteronism[J]. Hypertension, 2018, 72(3): 641-649. doi: 10.1161/HYPERTENSIONAHA.118.11382
-
图(1)
表(4)
计量
- 文章访问数: 714
- PDF下载数: 234
- 施引文献: 0