
Correlation between the diagnosis and prognosis of renal carcinoma and perirenal adipose based on parameters in CT imaging
-
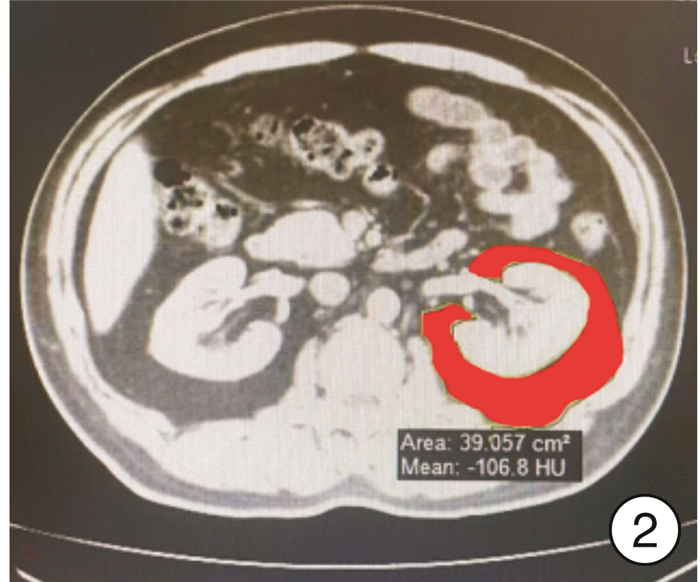
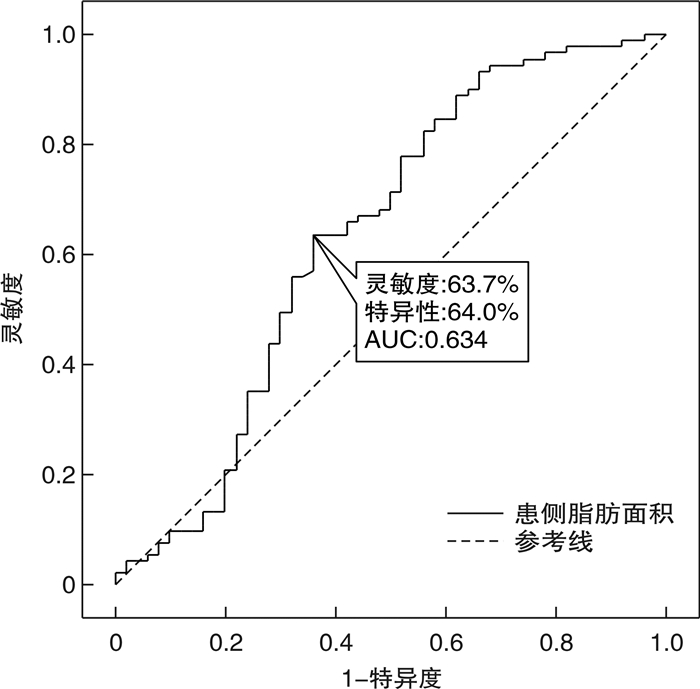
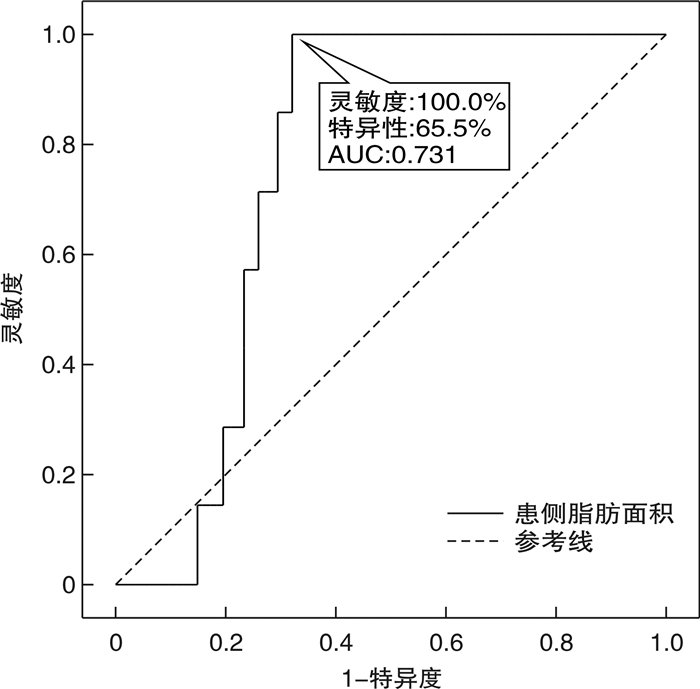
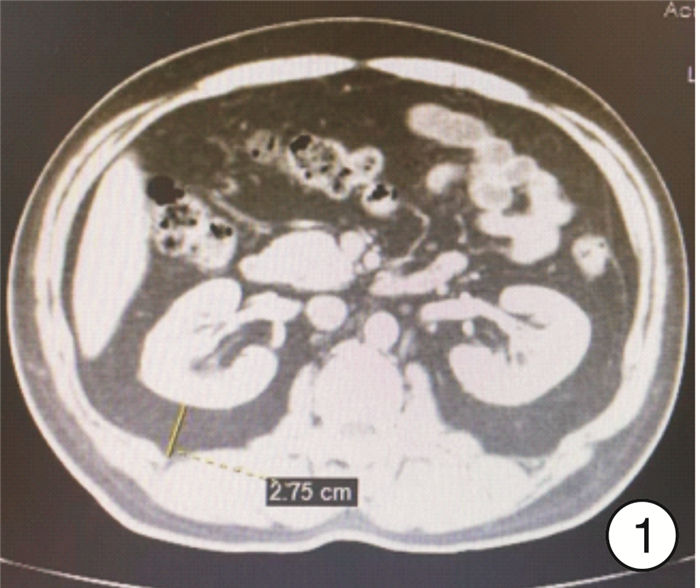
摘要: 目的 探究肾周脂肪CT参数对肾癌诊断和预后的临床意义和预测价值。方法 收集蚌埠医学院第一附属医院泌尿外科肾癌患者91例,同时收集50例肾囊肿患者作为对照。记录2组患者一般临床资料、MAP评分、肾周脂肪CT值、厚度和面积等资料,寻找对肾癌诊断具有临床意义的指标并分析其与肾癌患者预后的相关性。结果 2组患者的患侧肾周脂肪面积及手术时间比较差异有统计学意义(P<0.05)。回归分析结果显示,患侧肾周脂肪面积与肾癌相关(P<0.05),且为肾癌发生的独立危险因素。ROC曲线分析结果显示,在肾癌组与肾囊肿组中,最佳临界值为14.575,灵敏度为63.7%,特异度为64.0%,约登指数为0.277,ROC曲线下面积为0.634。在肾癌复发组与未复发组中,最佳临界值为21.485,灵敏度为100.0%,特异度为65.5%,约登指数为0.655,ROC曲线下面积为0.731。免疫组化结果表明高面积组解偶连蛋白1(uncoupling protein 1,UCP-1)表达显著高于低面积组。结论 本研究证实患侧肾周脂肪面积在肾癌诊断及预后判断方面具有一定的临床价值,值得关注并推广。Abstract: Objective To explore the clinical significance and predictive value of perirenal fat CT parameters in the diagnosis and prognosis of renal carcinoma.Methods We collected 91 patients with renal carcinoma, and 50 patients with renal cyst were collected as control. The general clinical data, MAP score, CT value of perirenal fat, thickness and area of patients were recorded to find clinically significant indicators for the diagnosis of renal cancer and analyze their correlation with the prognosis of patients with renal cancer.Results The perirenal fat area and operation time of the two groups were statistically significant(P < 0.05). The results of regression analysis showed that perirenal fat area was correlated with renal cancer(P < 0.05), and was also an independent risk factor for renal cancer. ROC curve analysis results showed that the optimal cut-off value was 14.575. The sensitivity was 63.7%, and the specificity was 64.0%. The Youden index was 0.277, and the area under ROC curve was 0.634 in the renal carcinoma group and the renal cyst group. In renal cancer recurrence group and non-recurrence group, the optimal cut-off value was 21.485. The sensitivity was 100.0%, and the specificity was 65.5%. The Youden index was 0.655, and the area under ROC curve was 0.731. Immunohistochemical results showed that UCP-1 expression in high area group was significantly higher than that in low area group.Conclusion This study confirmed that the perirenal fat area of the affected side has certain clinical value in the diagnosis and prognosis of renal cancer, which is worthy of attention and promotion.
-
Key words:
- renal cell cancer /
- perirenal adipose /
- browning
-

-
表 1 肾癌组和肾囊肿组资料比较
例(%),X±S,M(Q1,Q3) 参数 肾癌组(91例) 肾囊肿组(50例) P值 年龄/岁 56(31,79) 58(30,77) 0.866 性别 0.627 男 53(58.21) 27(54.00) 女 38(41.76) 23(46.00) 糖尿病 13(14.29) 3(6.00) 0.138 高血压 44(48.35) 19(38.00) 0.237 术前肌酐/(μmol/L) 74(63.00,83.00) 67(57.00,76.75) 0.059 MAP评分 0.496 轻 38(41.76) 22(44.00) 中 31(34.06) 20(40.00) 重 22(24.18) 8(16.00) 肿物直径/mm 4.69±1.43 4.67±1.23 0.948 手术时间/min 91.71±26.37 64.36±13.11 <0.001 患侧肾周脂肪CT值 -85.70(-93.70,-78.40) -88.90(-94.35,-82.15) 0.277 健侧肾周脂肪CT值 -86.50(-93.30,-77.70) -87.95(-95.03,-79.60) 0.620 患侧肾周脂肪厚度/cm 1.35±0.70 1.37±0.88 0.102 健侧肾周脂肪厚度/cm 1.13±0.60 1.13(0.60,1.82) 0.651 双侧肾周脂肪厚度之和/cm 2.48±1.20 2.24(1.26,3.72) 0.928 患侧肾周脂肪面积/cm2 18.64±9.79 12.18(4.41,22.80) 0.009 健侧肾周脂肪面积/cm2 15.95±8.99 11.04(5.98,20.55) 0.115 双侧肾周脂肪面积之和/cm2 34.59±18.64 28.23±21.17 0.067  下载: 导出CSV
下载: 导出CSV
表 2 2组间单因素和多因素logistic回归分析
因素 单因素分析 多因素分析 OR(95%CI) P值 OR(95%CI) P值 年龄 1.006(0.974~1.038) 0.727 性别 0.842(0.420~1.686) 0.627 糖尿病 2.611(0.707~9.644) 0.150 高血压 1.527(0.756~3.087) 0.238 术前肌酐 1.022(0.999~1.046) 0.055 MAP评分 1.194(0.759~1.879) 0.443 肿物直径 1.009(0.782~1.301) 0.947 手术时间 0.987(0.975~0.999) 0.035 0.984(0.972~0.997) 0.015 患侧肾周脂肪CT值 1.017(0.987~1.048) 0.265 健侧肾周脂肪CT值 0.995(0.979~1.012) 0.576 患侧肾周脂肪厚度 0.973(0.620~1.527) 0.906 健侧肾周脂肪厚度 0.738(0.454~1.202) 0.223 双侧肾周脂肪厚度之和 0.917(0.716~1.174) 0.491 患侧肾周脂肪面积 1.040(1.004~1.078) 0.030 1.048(1.009~1.088) 0.014 健侧肾周脂肪面积 1.018(0.979~1.057) 0.371 双侧肾周脂肪面积之和 1.015(0.997~1.035) 0.108
下载: 导出CSV
-
[1] Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2021[J]. CA Cancer J Clin, 2021, 71(1): 7-33. doi: 10.3322/caac.21654
[2] Lin WH, Yang ZG, Yan L, et al. Comparison of partial nephrectomy and radical nephrectomy for cystic renal cell carcinoma: a SEER-based and retrospective study[J]. Sci Rep, 2023, 13(1): 8052. doi: 10.1038/s41598-023-34950-x
[3] Lucocq J, Pillai S, Oparka R, et al. Complex renal cysts(Bosniak ≥ⅡF): interobserver agreement, progression and malignancy rates[J]. Eur Radiol, 2021, 31(2): 901-908. doi: 10.1007/s00330-020-07186-w
[4] 胡威, 祝恒成. 囊性肾癌的诊断和治疗现状分析[J]. 现代泌尿生殖肿瘤杂志, 2022, 14(3): 129-132. https://www.cnki.com.cn/Article/CJFDTOTAL-PXDM202203001.htm
[5] Huang HC, Chen S, Li W, et al. High perirenal fat thickness predicts a poor progression-free survival in patients with localized clear cell renal cell carcinoma[J]. Urol Oncol, 2018, 36(4): 157.e1-157.e6. doi: 10.1016/j.urolonc.2017.12.011
[6] 翁同辉, 任轲, 陈晗, 等. 内脏脂肪面积与肾癌病理分型及分级的相关性[J]. 现代泌尿外科杂志, 2021, 26(4): 322-327.
[7] Li XQ, Wang GC, Liu J, et al. Increased UCP1 expression in the perirenal adipose tissue of patients with renal cell carcinoma[J]. Oncol Rep, 2019, 42(5): 1972-1980.
[8] Jovanović M, Kovačević S, Brkljačić J, et al. Oxidative Stress Linking Obesity and Cancer: Is Obesity a 'Radical Trigger' to Cancer?[J]. Int J Mol Sci, 2023, 24(9): 8452. doi: 10.3390/ijms24098452
[9] Roopakala MS, Suresh A, Ashtalakshmi, et al. Anthropometric measurements as predictors of intraabdominal fat thickness[J]. Indian J Physiol Pharmacol, 2009, 53(3): 259-264.
[10] Wu HY, Xu SY, Chen LL, et al. Waist to height ratio as a predictor of abdominal fat distribution in men[J]. Chin J Physiol, 2009, 52(6): 441-445. doi: 10.4077/CJP.2009.AMH064
[11] Kojima S, Usui N, Shigetake M, et al. Intramuscular and abdominal fat measured by computed tomography and mortality of hemodialysis patients[J]. Nephrol Dial Transplant, 2023: gfad169. doi: 10.1093/ndt/gfad169
[12] Vural M, Akdal Dolek B, Ucar O, et al. The evaluation of subcutaneous and visceral adipose tissue changes by computed tomography in coronavirus disease 2019 and comparison with quantitative analysis of lung involvement[J]. Curr Med Imaging, 2023.
[13] Jespersen NZ, Feizi A, Andersen ES, et al. Heterogeneity in the perirenal region of humans suggests presence of dormant brown adipose tissue that contains brown fat precursor cells[J]. Mol Metab, 2019, 24: 30-43. doi: 10.1016/j.molmet.2019.03.005
[14] Adamczak M, Wiecek A. The adipose tissue as an endocrine organ[J]. Semin Nephrol, 2013, 33(1): 2-13. doi: 10.1016/j.semnephrol.2012.12.008
[15] Di WJ, Zhang WL, Zhu B, et al. Colorectal cancer prompted adipose tissue browning and cancer cachexia through transferring exosomal miR-146b-5p[J]. J Cell Physiol, 2021, 236(7): 5399-5410. doi: 10.1002/jcp.30245
[16] Zhang HY, Zhu L, Bai M, et al. Exosomal circRNA derived from gastric tumor promotes white adipose browning by targeting the miR-133/PRDM16 pathway[J]. Int J Cancer, 2019, 144(10): 2501-2515. doi: 10.1002/ijc.31977
[17] Wei G, Sun HL, Dong K, et al. The thermogenic activity of adjacent adipocytes fuels the progression of ccRCC and compromises anti-tumor therapeutic efficacy[J]. Cell Metab, 2021, 33(10): 2021-2039.e8. doi: 10.1016/j.cmet.2021.08.012
[18] Aurilio G, Piva F, Santoni M, et al. The role of obesity in renal cell carcinoma patients: clinical-pathological implications[J]. Int J Mol Sci, 2019, 20(22): 5683. doi: 10.3390/ijms20225683
[19] Fan WL, Yeh YM, Liu TT, et al. Leptin is associated with poor clinical outcomes and promotes clear cell renal cell carcinoma progression[J]. Biomolecules, 2021, 11(3): 431. doi: 10.3390/biom11030431
[20] Sun GX, Zhang XM, Liu ZH, et al. The adiponectin-AdipoR1 axis mediates tumor progression and tyrosine kinase inhibitor resistance in metastatic renal cell carcinoma[J]. Neoplasia, 2019, 21(9): 921-931. doi: 10.1016/j.neo.2019.07.004
-

图(5)
表(2)
计量
- 文章访问数: 783
- PDF下载数: 304
- 施引文献: 0