
Clinical efficacy of transumbilical single-port laparoscopy combined with ureteroscopy versus conventional laparoscopy in the treatment of upper and middle ureteral stenosis
-
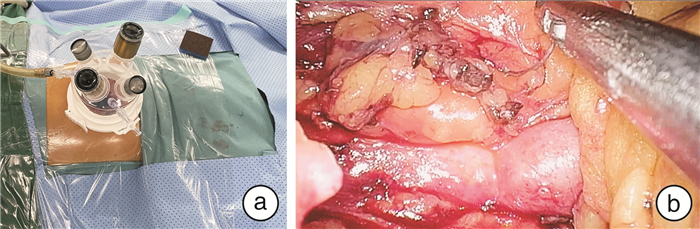
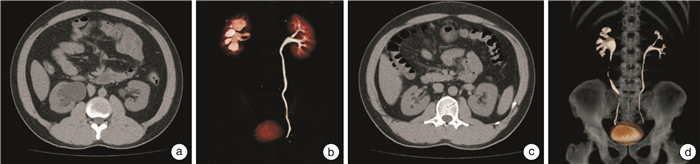
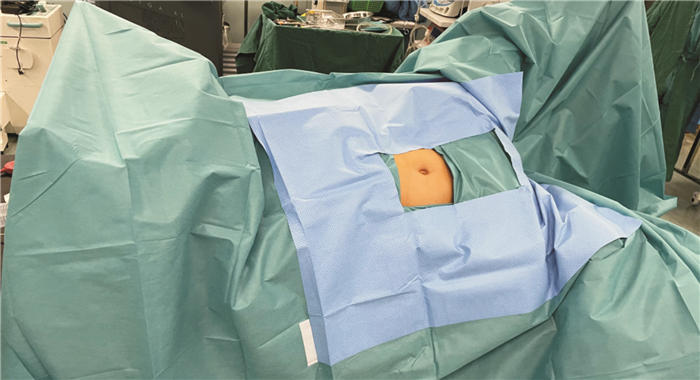
摘要: 目的 探讨经脐单孔腹腔镜联合输尿管镜治疗中上段输尿管狭窄的可行性及术后疗效观察。方法 回顾性分析2020年4月—2022年3月南方医科大学第三附属医院收治的35例因输尿管狭窄行输尿管狭窄段切除后再吻合术患者的临床资料。其中单孔腹腔镜联合输尿管镜组患者25例,传统腹腔镜组10例。术中采用斜卧截石位,单孔腹腔镜联合输尿管镜组手术采用脐部约3 cm切口,放置四通道单孔穿刺套件,用于放置腹腔镜观察孔及操作孔,术中根据输尿管镜精准定位输尿管狭窄段及留置输尿管内支架管。与传统腹腔镜组比较分析相关手术指标、术后并发症、患者满意度等临床数据。结果 所有患者均顺利完成手术,单孔腹腔镜联合输尿管镜组术中无增加辅助孔或改开放手术,单孔腹腔镜联合输尿管镜组平均手术时间(125.41±42.07) min,术后平均住院时间为(7.67±3.42) d,与传统腹腔镜组比较差异无统计学意义。2组患者围手术期无明显并发症发生,随访1年以上,患者肾积水较前减轻,肾功能得以改善。此外,单孔腹腔镜联合输尿管镜组部分不留置术腔引流管,患者手术切口美观,满意度好。结论 单孔腹腔镜联合输尿管镜治疗输尿管中上段狭窄是安全可行的,并且具有术后恢复快、美容效果好等优势。对于具有一定腹腔镜技术经验的术者是一种临床可选择的手术方式。Abstract: Objective To explore the feasibility and postoperative efficacy of transumbilical single port laparoscopy combined with ureteroscopy in the treatment of upper and middle ureteral stenosis.Methods The case data of 35 patients admitted to our hospital from April 2020 to March 2022 for ureteral stenosis who underwent ureteral stenosis segment resection followed by reanastomosis were retrospectively analyzed. There were 25 patients in the single-port laparoscopy combined with ureteroscopy group and 10 patients in the conventional laparoscopy group. The operation was performed in a reclined lithotomy position, and the single-port laparoscopy group was operated with an umbilical incision of about 3 cm. A four-channel single-port puncture kit was used for placing the laparoscopic observation holes and operation holes, and the ureteral stents were precisely localized according to the ureteroscopy and left in place. Clinical data such as relevant surgical indexes, postoperative complications, and patient satisfaction were analyzed in comparison with the traditional laparoscopic group.Results All patients were successfully completed the operation, and patients in the single-port laparoscopic group didn't experience intraoperative additional auxiliary holes or conversion to open surgery. The operation time of the single-port laparoscopic group was (125.41±42.07) min, and the length of postoperative hospitalization was (7.67±3.42) d. The differences were not statistically significant when comparing with those of the traditional laparoscopic group. There were no obvious complications during the perioperative period in the two groups. After more than 1 year of follow-up period, the patients' hydronephrosis was reduced, and the renal function was improved. In addition, postoperative drainage tubes weren't indwelt in some of the patients in the single-port laparoscopic group, and the patients' surgical incisions were beautiful and satisfactory.Conclusion Single-port laparoscopy combined with ureteroscopy is safe and feasible for the treatment of upper and middle ureteral stenosis and has the advantages of fast postoperative recovery and good cosmetic results. It is a clinical option for operators with some experience in laparoscopic techniques.
-
Key words:
- ureteral stenosis /
- single-port laparoscopy /
- ureteroscopy
-

-
表 1 患者术前一般特征资料
例(%),X±S,M(P25,P75) 项目 单孔腹腔镜联合输尿管镜组(25例) 传统腹腔镜组(10例) 年龄/岁 36(16,67) 39(26,57) 性别 男 19(76.0) 4(40.0) 女 6(24.0) 6(60.0) BMI/(kg/m2) 22.46 (20.49,25.64) 21.73 (19.76,24.13) 既往结石病史 9(36.0) 6(60.0) 患侧 右侧 14(56.0) 4(40.0) 左侧 11(44.0) 6(60.0) 狭窄原因 结石及反复腔内手术 9(36.0) 6(60.0) 腹腔术后粘连压迫 2(8.0) 2(20.0) 输尿管走行异常 2(8.0) 1(10.0) 输尿管息肉 3(12.0) 0(0) 其他 9(36.0) 1(10.0) 狭窄长度/cm 1.07±0.72 1.25±0.61 <1 13(52.0) 4(40.0) ≥1 12(48.0) 6(60.0) 既往腹腔手术史 2(8.0) 2(2.0)  下载: 导出CSV
下载: 导出CSV
表 2 2组术中及术后比较
X±S,M(P25,P75) 指标 单孔腹腔镜联合输尿管镜组(25例) 传统腹腔镜组(10例) P值 手术时间/min 125.41±42.07 123.57±40.49 0.931 预计出血量/mL 50(20,80) 50(20,100) 0.845 VAS评分/分 1.13±0.53 1.46±0.61 0.124 术后卧床时间/h 20.71 (16.69,35.83) 22.89 (17.76,37.43) 0.738 术后住院时间/d 7(5,8.25) 7(4,9.5) 0.892 术后带管时间/d 71(59.25,86) 77(60.5,88.75) 0.743 美容效果评分/分 4.51±1.16 3.67±1.02 0.047 注:VAS为视觉模拟评分。
下载: 导出CSV
表 3 2组术前、术后肌酐水平恢复比较
μmol/L,X±S 时间 单孔腹腔镜联合输尿管镜组(25例) 传统腹腔镜组(10例) 术前 117.43±86.37 131.9±83.97 术后 96.52±76.81 116.5±78.62 t 7.779 6.843 P值 <0.01 <0.01
下载: 导出CSV
-
[1] Vorobev V, Beloborodov V, Golub I, et al. Urinary System Iatrogenic Injuries: Problem Review[J]. Urol Int, 2021, 105(5-6): 460-469.
[2] Li X, Qiao J, Xiong S, et al. The surgical outcomes of reconstruction for the treatment of ureteral stricture after holmium laser lithotripsy: The comprehensive experiences[J]. Asian J Surg, 2022, 45(12): 2713-2718.
[3] 廖文彪, 杨嗣星, 宋超, 等. 输尿管镜钬激光碎石术后输尿管狭窄的处理方法5年单中心回顾性研究[J]. 中华泌尿外科杂志, 2021, 42(12): 910-914.
[4] Kapogiannis F, Spartalis E, Fasoulakis K, et al. Laparoscopic and Robotic Management of Ureteral Stricture in Adults[J]. In Vivo, 2020, 34(3): 965-972. doi: 10.21873/invivo.11864
[5] Buffi NM, Lughezzani G, Hurle R, et al. Robot-assisted Surgery for Benign Ureteral Strictures: Experience and Outcomes from Four Tertiary Care Institutions[J]. Eur Urol, 2017, 71(6): 945-951. doi: 10.1016/j.eururo.2016.07.022
[6] 钟子芳, 伍耿青, 廖汉清, 等. 输尿管狭窄腔内治疗新进展[J]. 江西医药, 2022, 55(7): 943-947. https://www.cnki.com.cn/Article/CJFDTOTAL-JXYY202007052.htm
[7] May PC, Hsi RS, Tran H, et al. The Morbidity of Ureteral Strictures in Patients with Prior Ureteroscopic Stone Surgery: Multi-Institutional Outcomes[J]. J Endourol, 2018, 32(4): 309-314. doi: 10.1089/end.2017.0657
[8] Wollin DA, Carlos EC, Tom WR, et al. Effect of Laser Settings and Irrigation Rates on Ureteral Temperature During Holmium Laser Lithotripsy, an In Vitro Model[J]. J Endourol, 2018, 32(1): 59-63. doi: 10.1089/end.2017.0658
[9] Parpala-Spårman T, Paananen I, Santala M, et al. Increasing numbers of ureteric injuries after the introduction of laparoscopic surgery[J]. Scand J Urol Nephrol, 2008, 42(5): 422-427. doi: 10.1080/00365590802025857
[10] Álvarez-Maestro M, Carrion DM, Rivas JG, et al. Laparoscopic ureteroureterostomy for treatment of retrocaval ureter[J]. Cent European J Urol, 2019, 72(1): 75.
[11] 张倩, 刘浩, 周昕, 等. 超声在儿童输尿管纤维上皮性息肉致肾积水术前诊断及预后评估中的价值[J]. 放射学实践, 2023, 38(9): 1195-1199. https://www.cnki.com.cn/Article/CJFDTOTAL-FSXS202309023.htm
[12] Torres Castellanos L, Moreno Bencardino MC, Bravo-Balado A, et al. Evaluation of the Efficacy and Safety of Laser versus Cold Knife Urethrotomy in the Management of Patients with Urethral Strictures: A Systematic Review and Meta-Analysis of Randomized Clinical Trials[J]. Urol Int, 2017, 99(4): 453-459. doi: 10.1159/000478026
[13] Kachrilas S, Bourdoumis A, Karaolides T, et al. Current status of minimally invasive endoscopic management of ureteric strictures[J]. Ther Adv Urol, 2013, 5(6): 354-365. doi: 10.1177/1756287213505671
[14] 刘存东, 周冉冉, 包继明. 单孔腹腔镜技术在泌尿外科的应用进展及展望[J]. 临床泌尿外科杂志, 2022, 37(1): 1-5. https://lcmw.whuhzzs.com/article/doi/10.13201/j.issn.1001-1420.2022.01.001
[15] Tyagi V, Pahwa M, Lodha P, et al. Robot-assisted laparoscopic ureteral reimplant: A single-center experience[J]. Indian J Urol, 2021, 37(1): 42-47.
[16] Tang ZY, Chen Z, He Y, et al. Laparoendoscopic single-site ureteroureterostomy with intraoperative retrograde ureteroscopy-assisted technique for benign proximal and middle ureteral strictures: a single-center experience[J]. J Laparoendosc Adv Surg Tech A, 2014, 24(7): 493-496.
[17] 王芳, 张莉亚, 梁涛, 等. 经脐单孔腹腔镜子宫肌瘤剔除术的学习曲线分析[J]. 中国临床医生杂志, 2023, 51(8): 1001-1004. https://www.cnki.com.cn/Article/CJFDTOTAL-ZLYS202308035.htm
[18] Zhu W, Xiong S, Wu Y, et al. Indocyanine green fluorescence imaging for laparoscopic complex upper urinary tract reconstructions: a comparative study[J]. Transl Androl Urol, 2021, 10(3): 1071-1079.
[19] Huh WK, Johnson JL, Elliott E, et al. Fluorescence Imaging of the Ureter in Minimally Invasive Pelvic Surgery[J]. J Minim Invasive Gynecol, 2021, 28(2): 332-341.e14.
[20] Buffi N, Cestari A, Lughezzani G, et al. Robot-assisted uretero-ureterostomy for iatrogenic lumbar and iliac ureteral stricture: technical details and preliminary clinical results[J]. Eur Urol, 2011, 60(6): 1221-1225.
-

图(4)
表(3)
计量
- 文章访问数: 371
- PDF下载数: 155
- 施引文献: 0