
Surgical protocol and experience of transurethral en-bloc resection of large non-muscle invasive bladder cancer
-
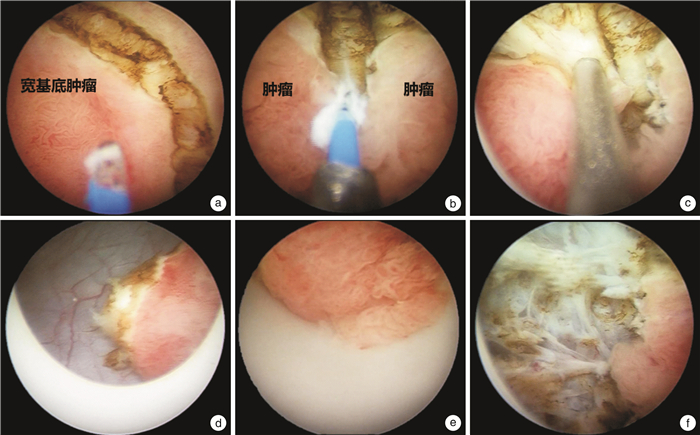
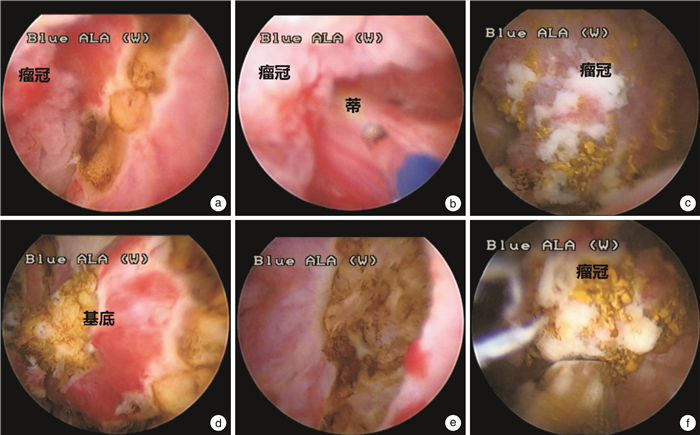
摘要: 目的 探讨经尿道膀胱肿瘤铥激光整块切除术治疗大体积(≥3 cm)非肌层浸润性膀胱癌的手术方法及其有效性和安全性。方法 回顾性分析2019年6月—2021年10月在华中科技大学同济医学院附属同济医院泌尿外科收治的31例大体积非肌层浸润性膀胱癌患者,其肿瘤最大径均≥3 cm。患者术前均接受磁共振检查,评分为VI-RADS 2分。肿瘤中位最大径3.5(3.0~6.0) cm。手术方案为:对于明显带蒂的肿瘤归类为2b型,采用铥激光于蒂处离断肿瘤,对肿瘤基底行整块切除,瘤冠予以组织粉碎器吸出;无蒂宽基底肿瘤归类为2c型,采用铥激光预分割后再分别行整块剜除和取出。结果 31例患者均顺利完成手术,中位手术时间为50(20~80) min。无患者需要中转为传统电切术。术中未出现明显膀胱穿孔和闭孔反射等并发症。所有患者术后肿瘤标本均包含固有肌层。Ta、Tis、T1期患者分别有23、2、6例;低级别尿路上皮癌8例,高级别尿路上皮癌23例;有7例患者接受二次电切,二次电切术后病理均未见癌;13例术后接受规律吉西他滨灌注,18例接受卡介苗膀胱灌注。中位随访12个月,1例Ta高级别肿瘤患者于术后12个月复发,1例T1高级别肿瘤患者于术后18个月复发,均再次接受经尿道膀胱肿瘤切除术,术后仍为非肌层浸润性膀胱癌并接受膀胱灌注治疗。结论 初步经验显示经尿道膀胱肿瘤整块切除术治疗大体积(≥3 cm)非肌层浸润性膀胱癌的手术方案是安全可行的。Abstract: Objective To evaluate the efficacy and safety of transurethral en-bloc resection for large (≥3 cm) non-muscle invasive bladder cancer (NMIBC) using thulium laser.Methods The data of 31 patients with large NMIBC who admitted to the Department of Urology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology from June 2019 to October 2021 were analyzed retrospectively. All patients underwent preoperative magnetic resonance examination, and classified as VI-RADS 2. The median maximum diameter of the tumor was 3.5 (3.0-6.0) cm. The surgical protocol: (1) The tumor with obvious stalk was classified as type 2b. Thulium laser was used to separate the tumor head and base at the stalk. And then the tumor base was en-bloc resected with laser, and the large tumor head was sucked out with a morcellator. (2) The broad basal sessile tumors were classified as type 2c, which were presegmented by thulium laser and then en-bloc resected separately.Results All the 31 patients underwent operation successfully, and the median operation time was 50 (20-80) min. There was no transfer of conventional TURBT during operation. There were no bladder perforation, obturator reflex, or other sever complications. Postoperative tumor specimens of all patients included muscularis propria. There were 23, 2 and 6 patients diagnosed with Ta, Tis, and T1 tumors, respectively. There were 23 cases of high-grade urothelial carcinoma and 8 cases of low-grade urothelial carcinoma. No residual cancer was found in the 7 patients who received second resection. Thirteen patients received regular gemcitabine intravesical therapy and 18 patients received BCG intravesical therapy. After a median follow-up of 12 (6-30) months, 1 patient with Ta high-grade tumor recurred 12 months after surgery, and 1 patient with T1 tumor recurred 18 months after surgery. Both patients underwent TURBT again. They were still diagnosed as NMIBC and received intravesical therapy postoperatively.Conclusion The preliminary experience of this study suggests that our en-bloc resection protocol for large (≥3 cm) NMIBC is safe and feasible.
-

-
[1] 黄健, 许传亮, 章小平. 膀胱癌诊断治疗指南[M]. 黄健. 2019版中国泌尿外科和男科疾病诊断治疗指南. 北京: 科学出版社, 2020: 27-84.
[2] Witjes JA, Bruins HM, Cathomas R, et al. European Association of Urology Guidelines on Muscle-Invasive and Metastatic Bladder Cancer: Summary of the 2020 Guidelines[J]. Eur Urol, 2021, 79(1): 82-104. doi: 10.1016/j.eururo.2020.03.055
[3] Yanagisawa T, Mori K, Motlagh RS, et al. En Bloc Resection for Bladder Tumors: An Updated Systematic Review and Meta-Analysis of Its Differential Effect on Safety, Recurrence and Histopathology[J]. J Urol, 2022, 207(4): 754-768. doi: 10.1097/JU.0000000000002444
[4] Mori K, D'Andrea D, Enikeev DV, et al. En Bloc Resection for Nonmuscle Invasive Bladder Cancer: Review of the Recent Literature[J]. Curr Opin Urol, 2020, 30(1): 41-47. doi: 10.1097/MOU.0000000000000697
[5] Territo A, Bevilacqua G, Meneghetti I, et al. En Bloc Resection of Bladder Tumors: Indications, Techniques, and Future Directions[J]. Curr Opin Urol, 2020, 30(3): 421-427. doi: 10.1097/MOU.0000000000000737
[6] Teoh JY, MacLennan S, Chan VW, et al. An International Collaborative Consensus Statement on En Bloc Resection of Bladder Tumour Incorporating Two Systematic Reviews, a Two-Round Delphi Survey, and a Consensus Meeting[J]. Eur Urol, 2020, 78(4): 546-569. doi: 10.1016/j.eururo.2020.04.059
[7] 胡恒龙, 李博亚, 孟晓岩, 等. 膀胱影像报告和数据系统对肌层浸润性膀胱癌的预测价值研究[J]. 中华泌尿外科杂志, 2019, 40(7): 503-506. https://www.cnki.com.cn/Article/CJFDTOTAL-YXZD202101011.htm
[8] 胡恒龙, 李博亚, 刘征, 等. 基于VI-RADS的个体化经尿道膀胱肿瘤整块切除术的初步应用经验[J]. 中华泌尿外科杂志, 2021, 42(3): 180-184.
[9] 毛俊杰, 孙圣坤, 徐阿祥, 等. 针状电极经尿道切除直径大于3 cm膀胱肿瘤的临床观察[J]. 现代泌尿外科杂志, 2019, 29(1): 52-54, 69. https://www.cnki.com.cn/Article/CJFDTOTAL-MNWK201901018.htm
[10] Li K, Xu Y, Tan M, et al. A Retrospective Comparison of Thulium Laser En Bloc Resection of Bladder Tumor and Plasmakinetic Transurethral Resection of Bladder Tumor in Primary Non-Muscle Invasive Bladder Cancer[J]. Lasers Med Sci, 2019, 34(1): 85-92. doi: 10.1007/s10103-018-2604-8
[11] 王振誉, 朱华, 张冰, 等. 经尿道钬激光整块切除术治疗非肌层浸润性膀胱癌的疗效分析[J]. 临床泌尿外科杂志, 2021, 36(10): 789-791, 795. https://www.cnki.com.cn/Article/CJFDTOTAL-LCMW202110007.htm
[12] 中华医学会泌尿外科学分会, 中国膀胱癌联盟. 非肌层浸润性膀胱癌二次电切中国专家共识[J]. 中华泌尿外科杂志, 2017, 38(8): 561-563.
[13] 王寅, 鲍玉海, 张洪泽, 等. 非肌层浸润膀胱尿路上皮癌选择再次经尿道电切术的评价[J]. 临床泌尿外科杂志, 2022, 37(5): 350-353. https://lcmw.whuhzzs.com/article/doi/10.13201/j.issn.1001-1420.2022.05.004
[14] Hu H, Zhou M, Yang B, et al. A Systematic Review on the Role of Repeat Transurethral Resection after Initial En Bloc Resection for Non-Muscle Invasive Bladder Cancer[J]. J Clin Med, 2022, 11(17): 5049.
[15] Zhou M, Yang B, Zhou S, et al. Will Repeat Resection after Initial Transurethral En Bloc Resection Benefit Patients with High-Risk Non-Muscle-Invasive Bladder Cancer? A Propensity Score Matching Analysis[J]. J Cancer Res Clin Oncol, 2022.
[16] Rice P, Somani BK. A Systematic Review of Thulium Fiber Laser: Applications and Advantages of Laser Technology in the Field of Urology[J]. Res Rep Urol, 2021, 13: 519-527.
[17] Wang W, Liu H, Xia S. Thulium Laser Treatment for Bladder Cancer[J]. Asian J Urol, 2016, 3(3): 130-133.
[18] Naselli A, Introini C, Germinale F, et al. En Bloc Transurethral Resection of Bladder Lesions: A Trick to Retrieve Specimens up to 4.5 cm[J]. BJU Int, 2012, 109(6): 960-963.
-
 下载:
下载:
图(2)
计量
- 文章访问数: 2821
- PDF下载数: 653
- 施引文献: 0