
Preliminary use of "one-stop" hybridization in renal tumors: DSA-guided balloon occlusion of the branch renal arteries in hybrid partial nephrectomy
-
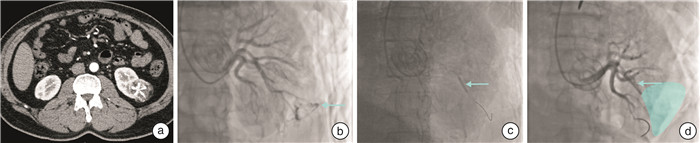
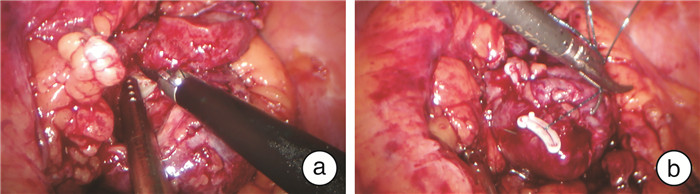
摘要: 目的 初步探讨数字减影血管造影(digital subtraction angiography,DSA)引导下肾分支动脉球囊阻断辅助肾部分切除的“一站式”杂交肾部分切除术(hybrid partial nephrectomy,HPN)的有效性及安全性。方法 总结华中科技大学同济医学院附属同济医院2021年8月—2021年10月采用DSA引导下肾分支动脉球囊阻断辅助肾部分切除的“一站式”杂交HPN治疗的3例肾肿瘤患者的临床资料。术前影像学检查均示T1a期肾占位性病变,R.E.N.A.L.评分分别为4、6、9分。手术过程如下:麻醉后行股动脉或桡动脉穿刺置入血管鞘备用,腹腔镜下直接打开肾周脂肪,充分显露肿瘤。随后在DSA引导下经动脉血管鞘置入导丝进入目标分支动脉,沿导丝置入球囊至目标肾分支动脉,在DSA监测下充起球囊并造影证实已阻断远端动脉血流。然后腹腔镜下切除肾肿瘤,常规缝合肾脏创面。DSA监测下收起球囊,再次造影证实分支动脉远端恢复血流且无造影剂溢出,直视下检查肾脏创面无渗血。结果 3例手术时长分别为95、118、127 min,其中热缺血时间(WIT)分别为18、17、23 min,术后标本可见肿瘤最大直径分别为1.5、2.4、3.8 cm,术后病理诊断分别为透明细胞癌(WHO/ISUP分级2级)、嫌色细胞性肾细胞癌、血管平滑肌脂肪瘤。3例患者术前与术后48 h血肌酐差值(δScr)分别为9、4、-2 μmol/L,术前与术后48 h估计肾小球滤过率差值(δeGFR)分别为10.9、3.3、-3.1 mL/min/1.73 m2。术后住院时间分别为4、5、4 d。结论 DSA引导下肾分支动脉球囊阻断辅助肾部分切除的“一站式”杂交手术是治疗局限性肾肿瘤安全可行的方法,其优点在于无须解剖肾门,精准地阻断肿瘤血供。Abstract: Objective To investigate the efficacy and safety of DSA interventional superselective segment artery balloon occlusion hybrid partial nephrectomy (DSB-HPN) as an adjunct to partial nephrectomy.Methods The clinical data of three patients with renal tumors treated by DSB-HPN in our hospital from August 2021 to October 2021 were summarized. The preoperative imaging showed a stage T1a renal tumor with R.E.N.A.L. scores of 4, 6, and 9, respectively. Following the administration of anesthesia, the femoral or radial artery is punctured and a vascular sheath is placed. Next, the perirenal fat is opened laparoscopically to completely expose the tumor. After that, under DSA guidance, a guidewire was inserted through the femoral artery sheath into the target renal segmental artery, and a balloon was placed along the guidewire. The balloon was inflated under DSA monitoring, and a renal arteriogram was completed to confirm the occlusion of the renal segmental artery flow. Then, a laparoscopic partial nephrectomy was performed, and the wound was sutured. The balloon was deflated under DSA monitoring and another angiogram was performed to confirm the restoration of blood flow of the distal target branch artery with no spillage of contrast material. Under direct laparoscope, the wound was re-examined to ensure no bleeding.Results The duration of surgery for the three patients was 95 min, 118 min, and 127 min, with a WIT of 18 min, 17 min, and 23 min, respectively. The maximum diameter of the tumor was 1.5 cm, 2.4 cm, and 3.8 cm, respectively. Their postoperative pathological diagnoses were clear cell renal carcinoma (WHO/ISUP grade 2), chromophobe renal cell carcinoma, and renal angiomyolipoma, respectively. The difference in blood creatinine (δScr) between preoperative and postoperative 48 h was 9 μmol/L, 4 μmol/L, and -2 μmol/L, respectively, and the difference in estimated glomerular filtration rate (δeGFR) was 10.9, 3.3, -3.1 mL/min/1.73 m2, respectively. The postoperative length of stays were 4 d, 5 d, and 4 d, for the three patients.Conclusion DSB-HPN is a safe and feasible way to treat limited renal tumors. The advantage of this procedure is that it does not require dissection of the renal hilum but can precisely occlude the tumor blood supply.
-

-
[1] Simone G, Gill IS, Mottrie A, et al. Indications, techniques, outcomes, and limitations for minimally ischemic and off-clamp partial nephrectomy: a systematic review of the literature[J]. Eur Urol, 2015, 68(4): 632-640.
[2] Thompson RH, Lane BR, Lohse CM, et al. Every minute counts when the renal hilum is clamped during partial nephrectomy[J]. Eur Urol, 2010, 58(3): 340-345.
[3] Shao PF, Qin C, Yin CJ, et al. Laparoscopic partial nephrectomy with segmental renal artery clamping: technique and clinical outcomes[J]. Eur Urol, 2011, 59(5): 849-855.
[4] Gallucci M, Guaglianone S, Carpanese L, et al. Superselective embolization as first step of laparoscopic partial nephrectomy[J]. Urology, 2007, 69(4): 642-645;discussion 645-646.
[5] D'Urso L, Simone G, Rosso R, et al. Benefits and shortcomings of superselective transarterial embolization of renal tumors before zero ischemia laparoscopic partial nephrectomy[J]. Eur J Surg Oncol, 2014, 40(12): 1731-1737.
[6] Liu FY, Yuan HJ, Li X, et al. Application of hypothermic perfusion via a renal artery balloon catheter during robot-assisted partial nephrectomy and effect on renal function[J]. Acad Radiol, 2019, 26(8): e196-e201.
[7] Maksimov AV, Martov AG, Pavlov LP. Renal function after laparoscopic partial nephrectomy with superselective balloon embolization of renal artery[J]. Urologiia, 2017(5): 21-25.
[8] Gill IS, Eisenberg MS, Aron M, et al. "Zero ischemia"partial nephrectomy: novel laparoscopic and robotic technique[J]. Eur Urol, 2011, 59(1): 128-134.
[9] Simone G, Capitanio U, Tuderti G, et al. On-clamp versus off-clamp partial nephrectomy: propensity score-matched comparison of long-term functional outcomes[J]. Int J Urol, 2019, 26(10): 985-991.
[10] 富智斌, 董凯, 顾迪, 等. 机器人辅助腹腔镜肾动脉无阻断肾部分切除术与分支阻断肾部分切除术治疗cT1期肾癌的疗效比较[J]. 临床泌尿外科杂志, 2021, 36(3): 173-177. https://lcmw.whuhzzs.com/article/doi/10.13201/j.issn.1001-1420.2021.03.002
[11] 田毅君, 屠晓华, 叶剑青, 等. 腹腔镜肾部分切除术中肾动脉损伤的处理[J]. 临床泌尿外科杂志, 2021, 36(8): 653-656. https://lcmw.whuhzzs.com/article/doi/10.13201/j.issn.1001-1420.2021.08.013
[12] Qian J, Jiang J, Li P, et al. Factors influencing the feasibility of segmental artery clamping during retroperitoneal laparoscopic partial nephrectomy[J]. Urology, 2019, 129: 92-97.
[13] Li P, Qin C, Cao Q, et al. A retrospective analysis of laparoscopic partial nephrectomy with segmental renal artery clamping and factors that predict postoperative renal function[J]. BJU Int, 2016, 118(4): 610-617.
[14] 韩松辰, 宋宇轩, 戴翔, 等. 热缺血时间对腹腔镜肾部分切除术后肾功能的影响[J]. 中华泌尿外科杂志, 2022, 43(5): 350-354. https://www.cnki.com.cn/Article/CJFDTOTAL-AZJZ202123011.htm
-
 下载:
下载:


图(4)
计量
- 文章访问数: 1475
- PDF下载数: 796
- 施引文献: 0