
Prediction model of the difficulty of adrenalectomy based on computed tomography parameters
-
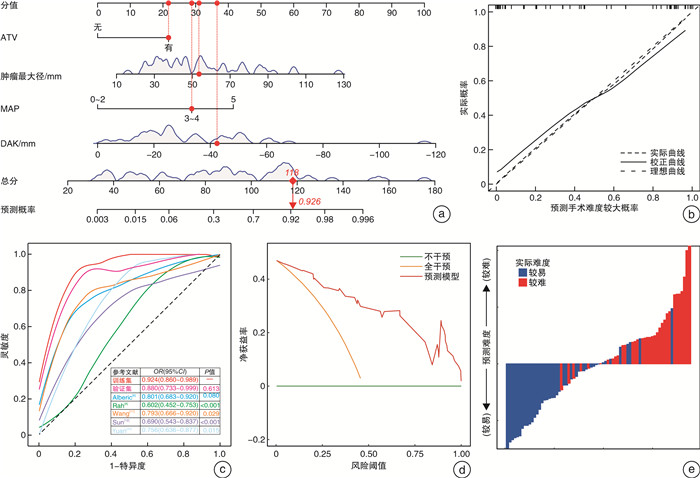
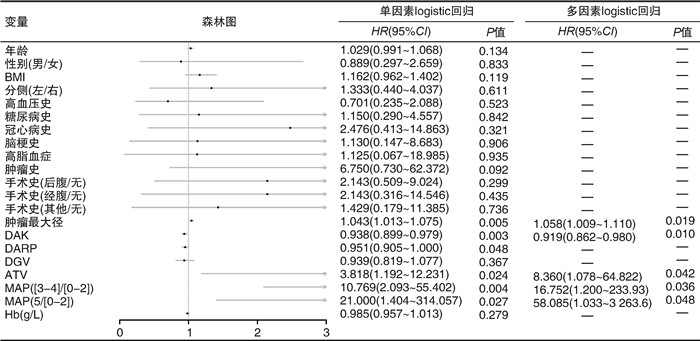
摘要: 目的 建立基于CT参数的肾上腺恶性肿瘤切除术难度预测模型,指导术者完善术前评估手术难度。方法 回顾性分析2014年8月—2021年12月就诊于山西白求恩医院并行手术治疗的75例肾上腺恶性肿瘤患者的临床资料。通过单因素logistic回归与逐步回归法多因素logistic回归筛选独立影响因素,构建列线图,采用ROC曲线分析列线图的预测效能,采用C指数和Bootstrap自抽样法验证列线图的区分度和一致性。结果 肾上腺恶性肿瘤切除术难度独立影响因素有:肿瘤最大径、梅奥评分、肿瘤血管贴附、肿瘤下极到肾上极的距离。根据筛选结果构建模型,C指数为0.924,临床决策曲线提示可提高25%的患者净获益率,说明模型预测效果良好。结论 肿瘤最大径、梅奥评分、肿瘤血管贴附、肿瘤下极到肾上极的距离是肾上腺恶性肿瘤切除术难度的独立影响因素,根据该结果构建的机器学习模型有着良好的预测性能,有助于术者评估手术难度,从而个体化完善术前准备,降低手术风险,提高患者获益。Abstract: Objective To establish a model to predict the difficulty of adrenalectomy based on computed tomography parameters and to guide the surgeons to improve the preoperative evaluation of the difficulty of adrenalectomy.Methods A retrospective analysis of 75 patients with malignant adrenal tumors treated in Shanxi Bethune Hospital from August 2014 to December 2021 was made. The independent influencing factors were screened by univariate logistic regression and stepwise multivariate logistic regression, and the nomogram was constructed. The ROC curve was used to analyze the prediction efficiency of the nomogram. The C-index and bootstrap self-sampling method were used to verify the discrimination and consistency of the nomogram.Results Adhesion of tumors to vessels, tumor diameter, distance from adrenal tumor to upper pole of kidney, and Mayo adhesive probability were selected as independent influencing factors. According to the results, the model was constructed. The C-index was 0.924. The decision curve analysis suggested that the net benefit rate of patients could be increased by about 25%, indicating that the prediction effect of the model was good.Conclusion Adhesion of tumors to vessels, tumor diameter, distance from adrenal tumor to upper pole of kidney, and Mayo adhesive probability are independent influencing factors in the difficulty of adrenalectomy for malignant tumors. The model based on the results has good predictive performance and is helpful for the surgeon to evaluate the difficulty of surgery to individualize and improve preoperative preparation, reduce the risk of surgery, and provide more benefit for patients.
-
Key words:
- adrenal glands /
- malignant neoplasms /
- prediction model /
- risk factors /
- nomogram
-

-
表 1 基线资料表
例(%),X±S,M(P25, P75) 变量 总队列(75例) 手术 t/Z/χ2 P值 较易(41例) 较难(34例) 术前参数 年龄/岁 48.55±15.75 46.56±15.74 50.94±15.64 -1.203 0.233 性别 0.054 0.817 男 43(57.3) 24(55.8) 19(44.2) 女 32(42.7) 17(53.1) 15(46.9) BMI/(kg/m2) 23.28±3.30 22.95±3.27 23.67±3.35 -0.938 0.351 患侧 0.001 0.980 左侧 31(41.3) 17(54.8) 14(45.2) 右侧 44(58.7) 24(54.5) 20(45.5) 高血压史 0.547 0.460 无 34(45.3) 17(50.0) 17(50.0) 有 41(54.7) 24(58.5) 17(41.5) 糖尿病史 0.300 0.584 无 62(82.7) 33(53.2) 29(46.8) 有 13(17.3) 8(61.5) 5(38.5) 冠心病史 0.068 0.794 无 68(90.7) 38(55.9) 30(44.1) 有 7(9.3) 3(42.9) 4(57.1) 脑梗史 0.009 0.924 无 67(89.3) 36(53.7) 31(46.3) 有 8(10.7) 5(62.5) 3(37.5) 高脂血症 0.001 0.999 无 71(94.7) 39(54.9) 32(45.1) 有 4(5.3) 2(50.0) 2(50.0) 肿瘤史 2.984 0.084 无 66(88.0) 39(59.1) 27(40.9) 有 9(12.0) 2(22.2) 7(77.8) 手术史 1.939 0.585 无 46(61.3) 28(60.9) 18(39.1) 后腹手术史 17(22.7) 8(47.1) 9(52.9) 经腹手术史 5(6.7) 2(40.0) 3(60.0) 其他手术史 7(9.3) 3(42.9) 4(57.1) 肿瘤最大径/mm 47.00(35.10,69.10) 40.80(32.00,52.00) 66.50(48.45,91.80) 4.326 < 0.001 DAK/mm -27.90(-48.80,-18.00) -23.20(-28.80,-14.40) -43.70(-52.57,-26.63) 3.672 < 0.001 DARP/mm 4.50(-3.90,14.40) 8.00(0.00,18.75) 0.80(-10.30,6.80) 3.065 0.002 DGV/mm 1.00(0.00,4.00) 2.00(0.00,5.00) 0.00(0.00,3.75) 1.804 0.059 ATV 6.776 0.009 无 41(54.7) 28(68.3) 13(31.7) 有 34(45.3) 13(38.2) 21(61.8) MAP/分 14.857 0.011 0 6(8.0) 6(100.0) 0(0) 1 4(5.3) 2(50.0) 2(50.0) 2 10(13.3) 9(90.0) 1(10.0) 3 35(46.7) 17(48.6) 18(51.4) 4 14(18.7) 6(42.9) 8(57.1) 5 6(8.0) 1(16.7) 5(83.3) 术前Hb/(g/L) 131.88±22.12 135.93±23.02 127.00±20.24 1.765 0.082 术中术后参数 手术时间/min 155.00(121.00,205.00) 125.00(96.00,151.00) 217.50(185.00,256.75) 5.955 < 0.001 出血量/mL 100.00(20.00,500.00) 30.00(0.00,100.00) 500.00(200.00,800.00) 6.125 < 0.001 切除范围 1.027 0.311 部分切 66(88.0) 38(57.6) 28(42.4) 全切 9(12.0) 3(33.3) 6(66.7) 术式 6.452 0.040 后腹腔镜 49(65.3) 31(63.3) 18(36.7) 经腹腹腔镜 16(21.3) 8(50.0) 8(50.0) 开放手术 10(13.3) 2(20.0) 8(80.0) 病理类型 6.042 0.049 PPGL 56(74.7) 35(62.5) 21(37.5) 皮质癌 12(16.0) 3(25.0) 9(75.0) 转移癌 7(9.3) 3(42.9) 4(57.1) 分组 0.246 0.620 训练集 53(70.7) 25(47.2) 28(52.8) 验证集 22(29.3) 9(40.9) 13(59.1)  下载: 导出CSV
下载: 导出CSV
-
[1] Barzon L, Sonino N, Fallo F, et al. Prevalence and natural history of adrenal incidentalomas[J]. Eur J Endocrinol, 2003, 149(4): 273-285.
[2] 李乐乐, 窦京涛, 谷伟军, 等. 1173例肾上腺意外瘤病因构成分析[J]. 中华医学杂志, 2014, 94(8): 587-590.
[3] Crona J, Beuschlein F. Adrenocortical carcinoma-towards genomics guided clinical care[J]. Nat Rev Endocrinol, 2019, 15(9): 548-560. doi: 10.1038/s41574-019-0221-7
[4] Mete O, Asa SL, Gill AJ, et al. Overview of the 2022 WHO Classification of Paragangliomas and Pheochromocytomas[J]. Endocr Pathol, 2022, 33(1): 90-114. doi: 10.1007/s12022-022-09704-6
[5] 中华医学会内分泌学分会. 嗜铬细胞瘤和副神经节瘤诊断治疗专家共识(2020版)[J]. 中华内分泌代谢杂志, 2020, 36(9): 737-750. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGGZ202108005.htm
[6] Alberici L, Paganini AM, Ricci C, et al. Development and validation of a preoperative"difficulty score"for laparoscopic transabdominal adrenalectomy: a multicenter retrospective study[J]. Surg Endosc, 2022, 36(5): 3549-3557. doi: 10.1007/s00464-021-08678-6
[7] Natkaniec M, Dworak J, Pȩdziwiatr M, et al. Patients criteria determining difficulty of the laparoscopic lateral transperitoneal adrenalectomy. A retrospective cohort study[J]. Int J Surg, 2017, 43: 33-37. doi: 10.1016/j.ijsu.2017.05.032
[8] Rah CS, Kim WW, Lee YM, et al. New predictive factors for prolonged operation time of laparoscopic posterior retroperitoneal adrenalectomy; retrospective cohort study[J]. Int J Surg, 2021, 94: 106113. doi: 10.1016/j.ijsu.2021.106113
[9] Vidal O, Saavedra-Perez D, Martos JM, et al. Risk factors for open conversion of lateral transperitoneal laparoscopic adrenalectomy: retrospective cohort study of the Spanish Adrenal Surgery Group(SASG)[J]. Surg Endosc, 2020, 34(8): 3690-3695. doi: 10.1007/s00464-019-07264-1
[10] Chen YF, Scholten A, Chomsky-Higgins K, et al. Risk factors associated with perioperative complications and prolonged length of stay after laparoscopic adrenalectomy[J]. JAMA Surg, 2018, 153(11): 1036-1041. doi: 10.1001/jamasurg.2018.2648
[11] Wang JY, Yang B, Sun SW, et al. Perioperative factors influencing the difficulty of retroperitoneal laparoscopic adrenalectomy: a single-center retrospective study[J]. BMC Urol, 2022, 22(1): 22. doi: 10.1186/s12894-022-00976-y
[12] Sun SW, Wang JY, Yang B, et al. A nomogram for evaluation and analysis of difficulty in retroperitoneal laparoscopic adrenalectomy: a single-center study with prospective validation using LASSO-logistic regression[J]. Front Endocrinol, 2022, 13: 1004112. doi: 10.3389/fendo.2022.1004112
[13] Davidiuk AJ, Parker AS, Thomas CS, et al. Mayo adhesive probability score: an accurate image-based scoring system to predict adherent perinephric fat in partial nephrectomy[J]. Eur Urol, 2014, 66(6): 1165-1171. doi: 10.1016/j.eururo.2014.08.054
[14] Gagner M, Lacroix A, Bolté E. Laparoscopic adrenalectomy in Cushing's syndrome and pheochromocytoma[J]. N Engl J Med, 1992, 327(14): 1033.
[15] Higashihara E, Tanaka Y, Horie S, et al. A case report of laparoscopic adrenalectomy[J]. Nihon Hinyokika Gakkai Zasshi Jpn J Urol, 1992, 83(7): 1130-1133.
[16] Gaur DD. Laparoscopic operative retroperitoneoscopy: use of a new device[J]. J Urol, 1992, 148(4): 1137-1139.
[17] Gaujoux S, Mihai R, joint working group of ESES and ENSAT. European Society of Endocrine Surgeons(ESES)and European Network for the Study of Adrenal Tumours(ENSAT)recommendations for the surgical management of adrenocortical carcinoma[J]. Br J Surg, 2017, 104(4): 358-376.
[18] Barczyński M, Konturek A, Nowak W. Randomized clinical trial of posterior retroperitoneoscopic adrenalectomy versus lateral transperitoneal laparoscopic adrenalectomy with a 5-year follow-up[J]. Ann Surg, 2014, 260(5): 740-747;discussion 747-748.
[19] 王康, 姚雪, 刘鹏, 等. 日间手术模式下后腹腔镜手术治疗肾上腺良性肿瘤的初步体会[J]. 临床泌尿外科杂志, 2021, 36(10): 802-805. https://lcmw.whuhzzs.com/article/doi/10.13201/j.issn.1001-1420.2021.10.010
[20] 徐鹏, 王远涛, 肖平, 等. 俯卧位后入路腹腔镜在肾上腺肿瘤手术中的应用[J]. 中华泌尿外科杂志, 2016, 37(6): 458-460.
[21] 侯倩, 张彪, 罗瑶, 等. 嗜铬细胞瘤诊断研究进展[J]. 临床泌尿外科杂志, 2022, 37(12): 946-951. https://lcmw.whuhzzs.com/article/doi/10.13201/j.issn.1001-1420.2022.12.012
[22] Kira S, Sawada N, Nakagomi H, et al. Mayo adhesive probability score is associated with the operative time in laparoscopic adrenalectomy[J]. J Laparoendosc Adv Surg Tech A, 2022, 32(6): 595-599.
[23] Kim S, Han HS, Choi Y, et al. Laparoscopic removal of retroperitoneal tumor with maneuver of hanging inferior vena cava[J]. Surg Endosc, 2018, 32(7): 3401.
[24] Yuan YQ, Feng HQ, Kang Z, et al. Mayo adhesive probability score is associated with perioperative outcomes in retroperitoneal laparoscopic adrenalectomy[J]. ANZ J Surg, 2022, 92(12): 3273-3277.
-
图(2)
表(1)
计量
- 文章访问数: 1386
- PDF下载数: 427
- 施引文献: 0