
Effect of high-risk pathological features on the prognosis of urothelial carcinoma of the bladder
-
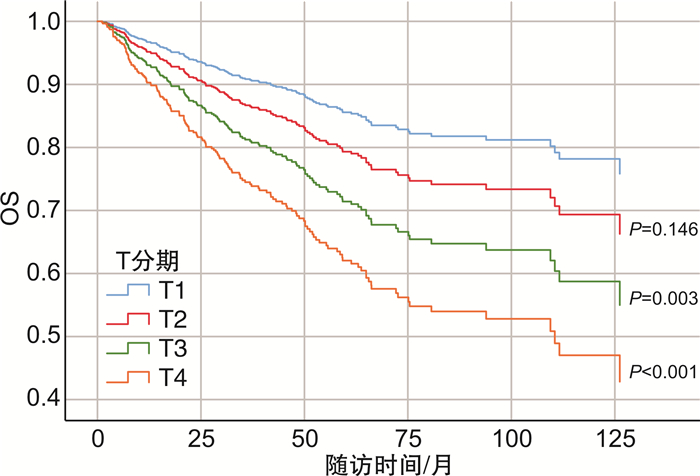
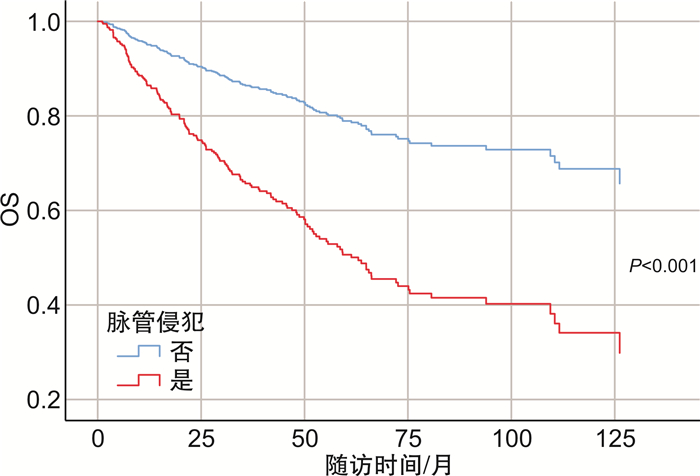
摘要: 目的 探讨膀胱癌患者根治性全切标本中不良病理学特征与患者预后的关系。方法 回顾性收集2006年1月1日—2023年12月1日于北京大学第一医院泌尿外科就诊并接受手术治疗患者的临床病理资料和预后信息,共纳入1 158例患者。主要研究终点为总生存期(overall survival,OS)。使用Kaplan-Meier法绘制生存曲线,采用单因素和多因素Cox比例风险回归模型评估患者不良病理学特征对患者预后的影响。结果 1 158例患者中男957例,女性201例;年龄22~92岁,中位年龄65.91(14)岁。平均随访时间39.75个月,性别(男vs女)、T分期(T2、T3、T4 vs T1)、淋巴结密度、鳞状化生、腺样分化、脉管侵犯和未分化癌是膀胱癌根治术后患者预后不良的独立危险因素(P < 0.05)。而WHO分级、肉瘤样分化、肿瘤坏死、神经浸润、前列腺尿道受累等组织病理学因素,与不伴有相应不良病理因素患者的OS相比,差异无统计学意义(P>0.05)。多因素Cox比例风险回归模型结果显示,T分期(T3、T4 vs T1)和脉管侵犯是OS的独立预后因素(P < 0.05)。结论 T分期(T3、T4 vs T1)和脉管侵犯是膀胱尿路上皮癌患者根治术后OS的独立预后因素,对术后高危患者的早期识别具有临床意义,并有助于指导进一步治疗。Abstract: Objective To investigate the relationship between adverse pathological features in bladder cancer patients and patients' prognosis.Methods Clinicopathological data and prognostic information of bladder cancer patients who were admitted to the Department of Urology at the Peking University First Hospital, and underwent radical cystectomy from January 1st, 2006 to December 1st, 2023 were retrospectively collected, and a total of 1 158 patients were included. The primary study endpoint was overall survival(OS). Survival curves were plotted using the Kaplan-Meier method, and the effect of adverse pathologic characteristics of patients on their prognosis was assessed using univariate and multivariate Cox proportional hazardous regression models.Results There were a total of 957 males and 201 females enrolled, aged 65.91(14) years(range: 22 to 92). The mean follow-up period was 39.75 months. Sex(male vs female), T stage(T2, T3, T4 vs T1), lymph node density, squamous metaplasia, adenoidal differentiation, vascular invasion, and undifferentiated carcinoma were independent risk factors in poor prognosis for bladder cancer patients after radical cystectomy(P < 0.05). In contrast, the histopathological factors such as WHO grade, sarcomatoid differentiation, tumor necrosis, nerve infiltration, and prostatic urethral involvement did not show statistically significant differences in OS compared with those of patients without the corresponding adverse pathological factors(P>0.05). The results of the multivariate Cox proportional hazardous regression model showed that patients' T stage(T3, T4 vs T1) and vascular invasion were independent prognostic factors in OS(P < 0.05).Conclusion T stage(T3, T4 vs T1) and vascular invasion are independent prognostic factors in OS for patients with urothelial carcinoma of the bladder after radical cystectomy, which is clinically significant for the early identification of high-risk postoperative patients and helps to guide further treatment.
-
Key words:
- urothelial carcinoma /
- bladder cancer /
- radical cystectomy /
- pathological features /
- prognosis
-

-
表 1 患者临床和病理学资料及OS预后因素的单因素及多因素分析结果
X±S,M(IQR) 项目 例数/值 单因素分析 多因素分析 HR(95%CI) P值 HR(95%CI) P值 性别 女 201 ~ 参考 ~ 参考 男 957 1.612(1.052~2.470) 0.028 1.490(0.897~2.477) 0.124 年龄/岁 65.91(14) 1.013(0.999~1.027) 0.064 T分期a) T1 285 ~ 参考 ~ 参考 T2 308 1.785(1.164~2.739) 0.008 1.430(0.883~2.317) 0.146 T3 293 2.698(1.764~4.127) < 0.001 2.088(1.276~3.418) 0.003 T4 173 3.951(2.534~6.159) < 0.001 2.865(1.703~4.824) < 0.001 Ta 13 0.584(0.080~4.275) 0.596 N分期b) 0 675 ~ 参考 1 66 1.363(0.712~2.607) 0.350 2 276 1.407(0.994~1.990) 0.054 淋巴结清扫总数/个 10.98(10) 1.012(0.996~1.028) 0.140 阳性淋巴结数/个 1.59(1) 1.035(0.997~1.074) 0.073 淋巴结密度 0.124±0.220 2.274(1.173~4.410) 0.015 1.510(0.747~3.053) 0.252 WHO分级c) G1 9 ~ 参考 G2 338 0.525(0.127~2.180) 0.375 G3 741 1.125(0.278~4.547) 0.869 肉瘤样分化 无 974 ~ 参考 有 184 1.279(0.870~1.879) 0.210 肿瘤坏死 无 872 ~ 参考 有 286 0.971(0.701~1.345) 0.860 鳞状化生 无 935 ~ 参考 ~ 参考 有 223 1.452(1.055~1.998) 0.022 1.121(0.776~1.620) 0.543 腺样分化 无 986 ~ 参考 ~ 参考 有 172 1.602(1.151~2.231) 0.005 1.040(0.706~1.532) 0.841 脉管侵犯 无 1 063 ~ 参考 ~ 参考 有 95 2.772(1.989~3.863) < 0.001 2.829(1.926~4.156) < 0.001 神经浸润 无 1 103 ~ 参考 有 55 1.636(0.865~3.094) 0.130 前列腺尿道受累 无 908 ~ 参考 有 250 1.247(0.907~1.715) 0.175 神经内分泌癌 无 1 140 ~ 参考 有 18 2.660(0.984~7.187) 0.054 未分化癌 无 1 152 ~ 参考 ~ 参考 有 6 5.186(1.653~16.271) 0.005 2.831(0.369~21.698) 0.317 原位癌 无 964 ~ 参考 有 194 1.051(0.736~1.501) 0.783 前列腺癌 无 858 ~ 参考 有 300 0.987(0.716~1.361) 0.936 注:a)T分期不详86例;b)N分期不详141例;c)WHO分级缺失70例。  下载: 导出CSV
下载: 导出CSV
-
[1] Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024[J]. CA Cancer J Clin, 2024, 74(1): 12-49. doi: 10.3322/caac.21820
[2] Rouprêt M, Seisen T, Birtle AJ, et al. European association of urology guidelines on upper urinary tract urothelial carcinoma: 2023 update[J]. Eur Urol, 2023, 84(1): 49-64. doi: 10.1016/j.eururo.2023.03.013
[3] Knowles M, Dyrskjøt L, Heath EI, et al. Metastatic urothelial carcinoma[J]. Cancer Cell, 2021, 39(5): 583-585. doi: 10.1016/j.ccell.2021.04.012
[4] Sánchez-Pellicer P, Boix-Rodríguez C, Hernández-Belmonte A, et al. Bladder cancer and probiotics: what do we know so far?[J]. Cancers(Basel), 2023, 15(23): 5551.
[5] 周佳维, 汪雄, 沈德贇, 等. 中性粒淋巴细胞比值与血小板淋巴细胞比值对腹腔镜膀胱癌根治术后肌层浸润性膀胱癌患者预后的预测价值[J]. 临床泌尿外科杂志, 2022, 37(2): 104-108. doi: 10.13201/j.issn.1001-1420.2022.02.006
[6] Witjes JA, Bruins HM, Carrión A, et al. European association of urology guidelines on muscle-invasive and metastatic bladder cancer: summary of the 2023 guidelines[J]. Eur Urol, 2024, 85(1): 17-31. doi: 10.1016/j.eururo.2023.08.016
[7] Flaig TW, Spiess PE, Abern M, et al. NCCN guidelinesⓇ insights: bladder cancer, version 2.2022[J]. J Natl Compr Canc Netw, 2022, 20(8): 866-878. doi: 10.6004/jnccn.2022.0041
[8] 张金英. 膀胱癌术后患者预后影响因素[J]. 中国老年学杂志, 2022, 42(4): 830-833. doi: 10.3969/j.issn.1005-9202.2022.04.018
[9] 周星宇, 侯亚坤, 木拉提·热夏提, 等. 膀胱癌根治术后患者的生存分析[J]. 西部医学, 2023, 35(11): 1679-1683. doi: 10.3969/j.issn.1672-3511.2023.11.022
[10] Zhang XP, Liu Q. Systemic immune inflammation index and T-staging predict prognosis in patients with muscle-invasive bladder cancer[J]. Arch Esp Urol, 2023, 76(7): 511-518. doi: 10.56434/j.arch.esp.urol.20237607.63
[11] 姚增文. 膀胱癌不同TNM分期对腹腔镜根治性膀胱切除术患者预后的影响[J]. 中国医疗器械信息, 2019, 25(2): 66-67. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGQX201902034.htm
[12] Yoneda K, Kamiya N, Utsumi T, et al. Impact of lymphovascular invasion on prognosis in the patients with bladder cancer-comparison of transurethral resection and radical cystectomy[J]. Diagnostics(Basel), 2021, 11(2): 244.
[13] Colomer Gallardo A, Candela L, Buisan Rueda O, et al. The Cancer of the Bladder Risk Assessment(COBRA)score accurately predicts cancer-specific survival after radical cystectomy: external validation and lymphovascular invasion assessment value to improve its performance[J]. Clin Genitourin Cancer, 2022, 20(3): 199-209. doi: 10.1016/j.clgc.2021.12.010
[14] Mitra AP, Cai J, Miranda G, et al. Management trends and outcomes of patients undergoing radical cystectomy for urothelial carcinoma of the bladder: evolution of the university of southern California experience over 3, 347 cases[J]. J Urol, 2022, 207(2): 302-313. doi: 10.1097/JU.0000000000002242
[15] Jaganmurugan R, Arora A, Chandankhede U, et al. Prognostic significance of lymph node density in pathological node positive urothelial carcinoma of the bladder-upfront surgery and post neoadjuvant chemotherapy cohorts[J]. Clin Genitourin Cancer, 2024, 22(2): 385-393.
[16] 白钰明, 张国文, 马可为, 等. 浸润性膀胱癌分子分型的预后研究及PD-L1的表达意义[J]. 临床泌尿外科杂志, 2022, 37(3): 184-188. doi: 10.13201/j.issn.1001-1420.2022.03.006
-
计量
- 文章访问数: 244
- 施引文献: 0